Why Erectile Dysfunction And Infertility Need A Natural Reset
When the reproductive system fails, the body has already filed a metabolic report.
A man does not usually arrive at erectile dysfunction through one failed night. He arrives after years of pressure inside blood vessels, sugar injury in small arteries, tobacco damage, abdominal fat, poor sleep, medication effects, untreated anxiety, or a heart-risk profile nobody connected to sex because nobody asked him the right question. By the time the penis refuses to hold blood, the vascular system may have been submitting evidence for years.
Infertility carries a similar deception. A woman may bleed every month and still fail to ovulate properly; she may ovulate and still have a damaged tube; she may have open tubes and still carry endometriosis, thyroid dysfunction, high prolactin, a distorted uterine cavity, or a male partner whose semen has never been tested because culture protected his pride longer than medicine protected her time. Month after month, disappointment is renamed patience when the file should already be open.
No serious fertility repair begins with herbs. It begins with a body audit: blood pressure, waist circumference, fasting glucose, HbA1c, lipid profile, semen analysis, cycle length, ovulation evidence, pelvic pain, sexual function, sleep quality, medication history, alcohol exposure, smoking, prior infection, miscarriage history, thyroid symptoms, prolactin symptoms, and age. Leave out the file, and the remedy becomes theater performed over unexamined disease.
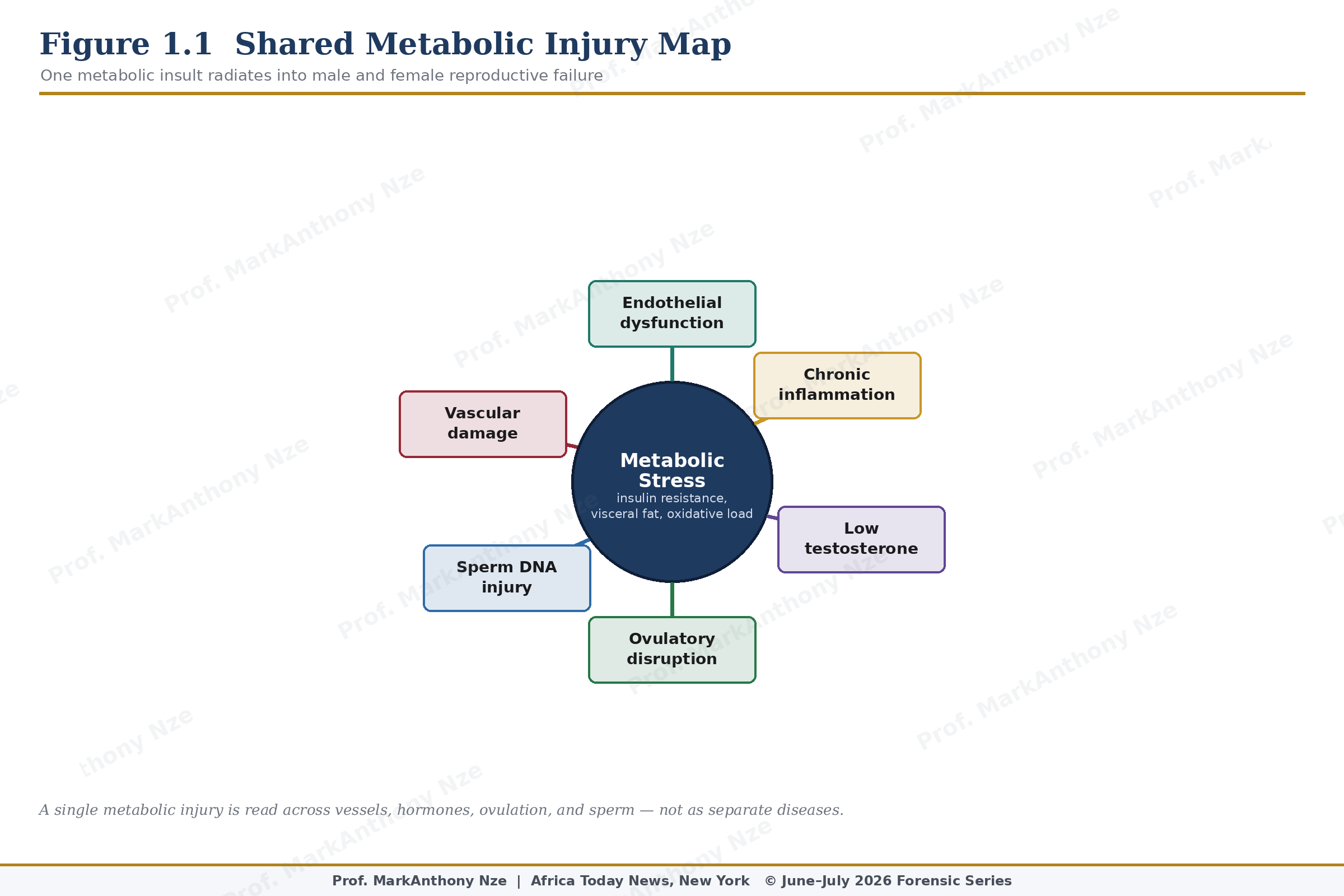
Figure 1.1. Shared Metabolic Injury Map.
Vascular injury explains much of the male side. An erection requires nitric oxide release, relaxation of smooth muscle inside the corpora cavernosa, rapid arterial inflow, venous trapping, intact nerve signaling, and enough hormonal and psychological stability for arousal to proceed. Diabetes, hypertension, dyslipidemia, smoking, obesity, metabolic syndrome, sleep apnea, depression, and cardiovascular disease can interfere with that sequence. A weak erection is not always a sexual event; at times, it is a circulatory report written in tissue.
Female fertility is less visible but equally unforgiving. A follicle must develop, ovulation must occur, sperm must arrive at the right time, a fallopian tube must permit encounter and transport, an embryo must reach the uterine cavity, and an endometrium must receive it. Thyroid function, prolactin level, insulin signaling, ovarian reserve, pelvic anatomy, endometriosis, semen quality, and timing can each damage that sequence. Calling the result unexplained too early is an error of investigation.
African households know the informal economy of reproductive panic. Roots are boiled, powders are mailed, capsules are praised by cousins who never saw a semen report, pastors are consulted, aunties accuse, and men disappear from testing while women carry the visible shame of an empty womb. That social pattern is not harmless background noise; it changes clinical timelines. A woman can lose a year to secrecy, another to imported supplements, another to prayer without semen analysis, and by then her ovaries have not waited politely.
Natural repair has a lawful place, but it must be stripped of fantasy. Food can alter insulin resistance, inflammatory load, lipid profile, oxidative stress, and body composition (Cristodoro et al., 2024). Exercise can improve vascular function and erectile scores (Rotimi et al., 2024) in some men, especially where ED carries cardiometabolic roots (Khera et al., 2023). Weight reduction may improve ovulatory pattern in women with metabolic disease or PCOS (Teede et al., 2023). Sleep repair may affect testosterone rhythm, appetite regulation, cortisol tone, and endocrine timing (Budihastuti et al., 2024). Smoking cessation removes vascular and gamete-level poison.
None of those interventions opens a blocked fallopian tube. None reverses severe azoospermia by force of optimism. None removes a cavity-distorting fibroid. None cures advanced endometriosis (Becker et al., 2022). None makes hidden sildenafil inside a so-called male-enhancement capsule safe. FDA warnings on sexual-enhancement products are not abstract regulatory gossip (U.S. Food and Drug Administration, 2026); they document a market where natural labels may conceal undeclared drug ingredients capable of dangerous interaction with nitrate medication or heart disease.
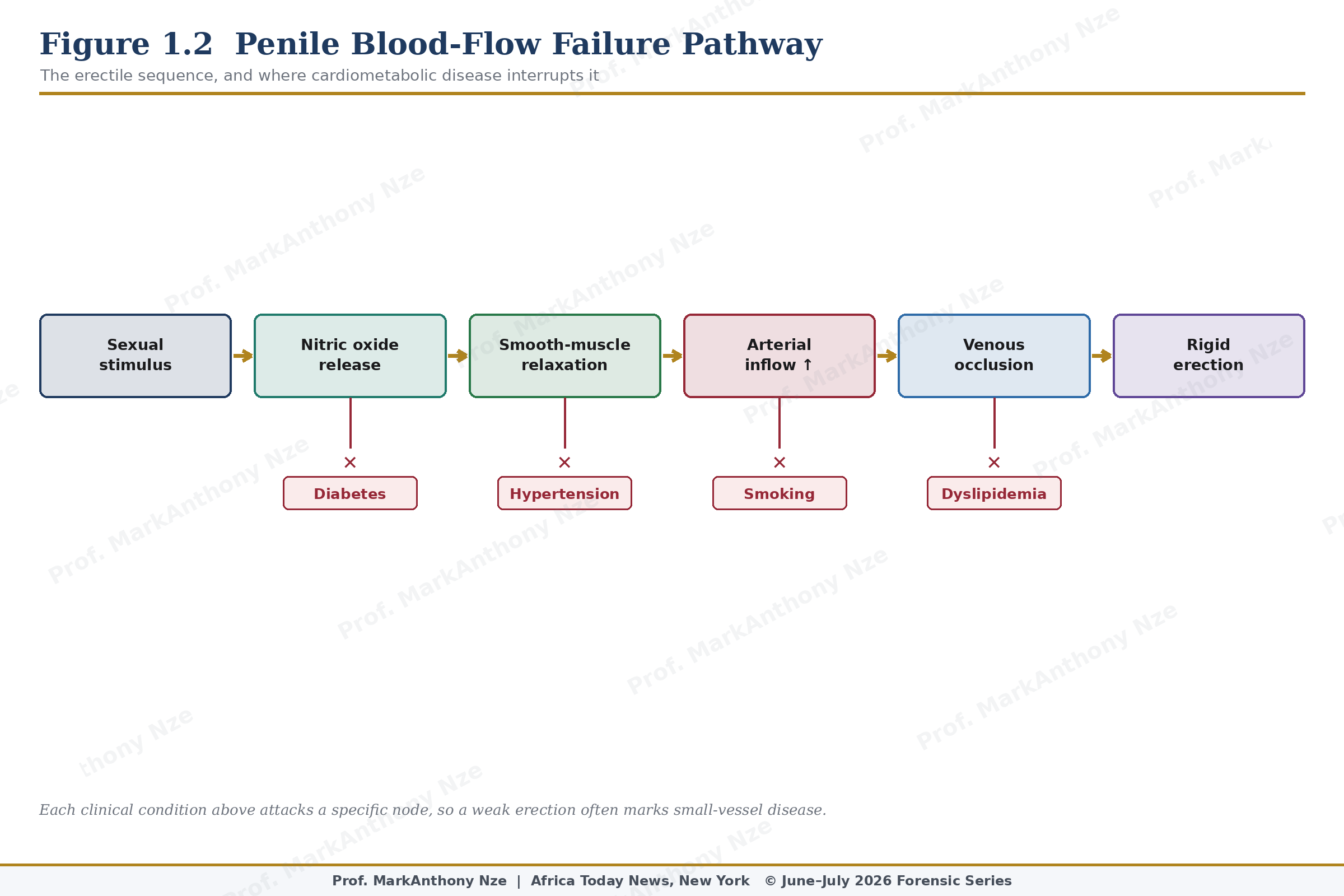
Figure 1.2. Penile Blood-Flow Failure Pathway.
Cardiometabolic disease often enters reproduction through quiet routes. Blood pressure may be high without headache, glucose may be abnormal without thirst, sleep apnea may occur without the patient calling it disease, and lipid injury may accumulate without pain. ED can expose these routes because penile circulation depends on small-vessel health. Infertility can expose them because ovulation, implantation, sperm production, and sexual function all respond to metabolic strain.
A couple trying to conceive must be treated as one diagnostic unit. Male fertility cannot be inferred from ejaculation, libido, beard growth, previous children, or sexual confidence. Semen analysis measures what culture cannot: concentration, total count, motility, morphology, volume, vitality (World Health Organization, 2021), and sometimes inflammatory clues. Female fertility cannot be inferred from monthly bleeding alone. Cycle length, ovulation evidence, pelvic pain, age, uterine structure, tubal risk, endocrine function, and miscarriage history all matter.
Diagnostic humility is not the same as pessimism. A low sperm count may improve after heat reduction, smoking cessation, weight repair, infection treatment, varicocele management (Brannigan et al., 2024), or stopping testosterone misuse, depending on cause. Irregular ovulation may improve when insulin resistance, sleep debt, excessive exercise, undernutrition, thyroid disease, or prolactin disturbance is corrected (Practice Committee of the American Society for Reproductive Medicine, 2024). Some problems remain stubborn despite repair. Honest medicine tells patients which category they are in as evidence appears.
Time changes the ethics of advice. A 27-year-old woman with regular cycles, no pelvic pain, no infection history, and a partner with normal semen may have room for structured timing and lifestyle repair. A 38-year-old woman with irregular cycles, severe menstrual pain, or repeated loss does not have the same margin. A 45-year-old man with diabetes, new ED, abdominal obesity, and poor sleep does not need a stamina capsule before cardiovascular review. Equal reassurance in unequal risk is bad triage.
A natural reset should last long enough to measure but not long enough to become avoidance. Ninety days is practical because sperm production, training adaptation, glucose control, sleep recovery, diet adherence, alcohol reduction, and exposure changes need time to show patterns. During those ninety days, the couple should not suspend medical evaluation when red flags are present. Tracking and testing can move together when neither is used to delay the other.
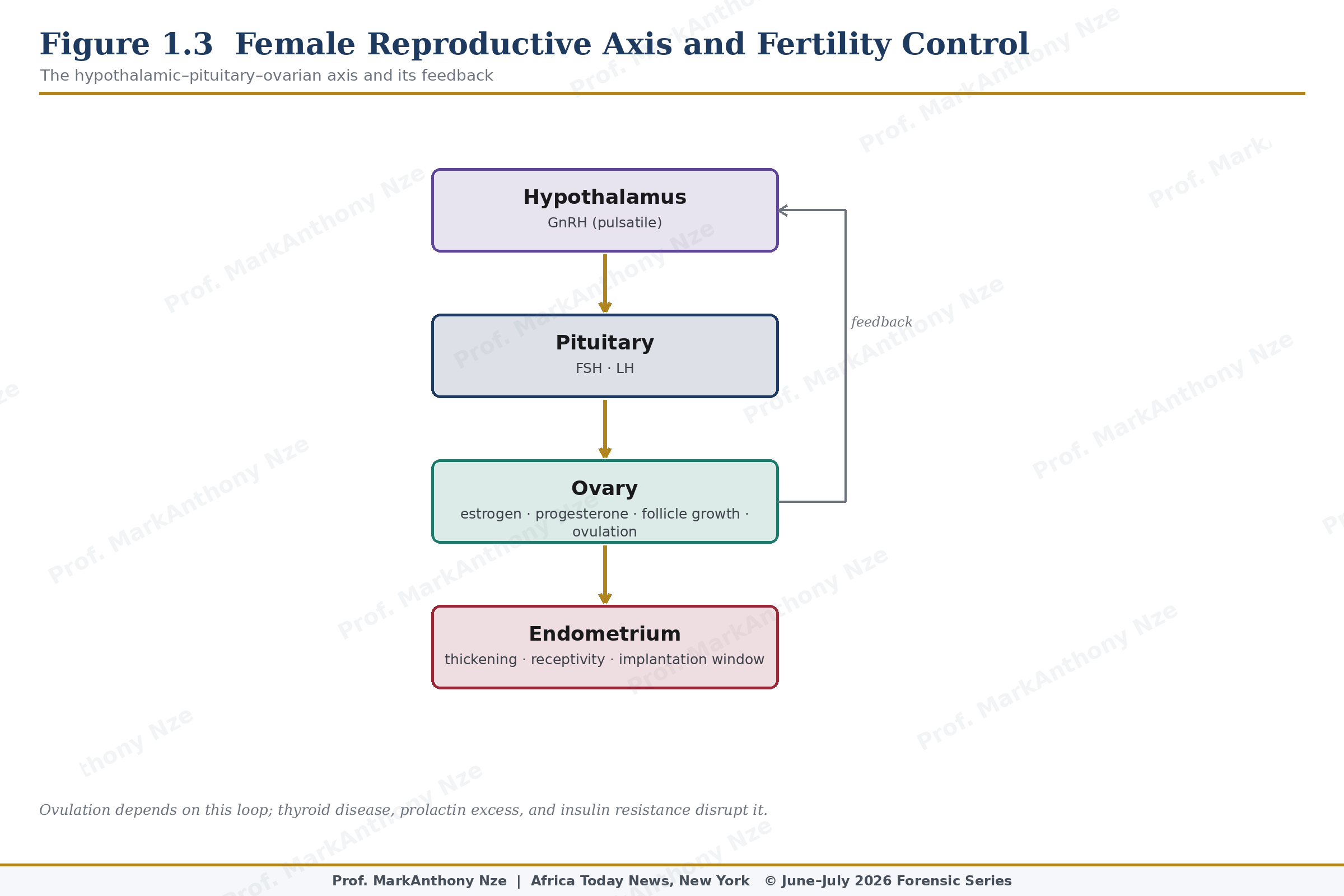
Figure 1.3. Female Reproductive Axis And Fertility Control.
Clinical honesty also protects against blame. Infertility is not divine punishment, female failure, male weakness, or ancestral revenge. Erectile dysfunction is not automatic proof of lost manhood. These are biological events occurring inside social systems that often reward silence and punish disclosure. Better medical writing must expose the conditions under which patients are pushed away from evidence and into the hands of sellers. Natural care is useful only after the body has been forced to testify.
A reader should leave this first article with one severe habit: ask what has been measured. If a man has ED, ask about blood pressure, glucose, lipids, sleep, medication, testosterone only when indicated, and cardiovascular risk. If a woman cannot conceive, ask about ovulation, age, pain, tubes, uterus, endocrine signs, miscarriage, and semen analysis. If a remedy is offered before those questions, demand the file.
Such discipline is not hostile to tradition. Many households already understand fasting, movement, herbs, rest, restraint, and sexual order as parts of health, but inherited practice must be tested against anatomy and risk. A plant may support nutrition or ritual confidence; it cannot replace a semen report, an ultrasound, a thyroid result, or an ECG when the symptoms point there. Respect is not obedience to error.
Repair begins when language changes. Bedroom failure becomes vascular evidence, delayed pregnancy becomes a shared investigation, and natural care becomes a measured intervention rather than a commercial promise wrapped around fear.
Clinic and household language must change together. A physician may order tests, but a family can still sabotage the plan by protecting the wrong secret. A man who refuses semen analysis and a seller who promises womb cleansing are working from different motives, yet both can delay the same woman. Natural repair begins only when the couple agrees that evidence outranks embarrassment.
Source & Clinical Standards
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.