Food, Blood Flow And Reproductive Power
Africa’s Leading Pioneer of Forensic Serial Journalism
Creator, NZE FORENSIC SERIAL JOURNALISM METHOD™
Diet works when it changes vessels, insulin, inflammation, and oxidative burden.
Food enters reproductive medicine because it is repeated exposure. Every day, vessels, ovaries, testes, liver, adipose tissue, gut microbiota, and endocrine pathways respond to what is eaten, how often it is eaten, and what metabolic state follows. A fertility diet is not a charm. It is an attempt to reduce vascular stress, glucose instability, inflammatory load, oxidative injury, nutrient deficiency, and weight-related endocrine pressure.
Male erectile function is especially sensitive to vascular nutrition. Diets that worsen insulin resistance, triglycerides, blood pressure, abdominal adiposity, and oxidative stress will not spare penile arteries because the patient feels young or culturally confident. A Mediterranean-style pattern has biologic plausibility because it supports cardiometabolic health through vegetables, legumes, fruit, fish, nuts, olive oil, whole grains, and reduced ultra-processed intake.
Female fertility also reads diet through several channels. Ovulation, follicular development, endometrial function, insulin sensitivity, thyroid support, inflammation, and body composition can all be affected by dietary quality. PCOS makes this relationship visible because insulin resistance can worsen androgen excess and ovulatory irregularity. A woman with irregular cycles does not need a punitive diet; she needs a metabolic plan that can be sustained.
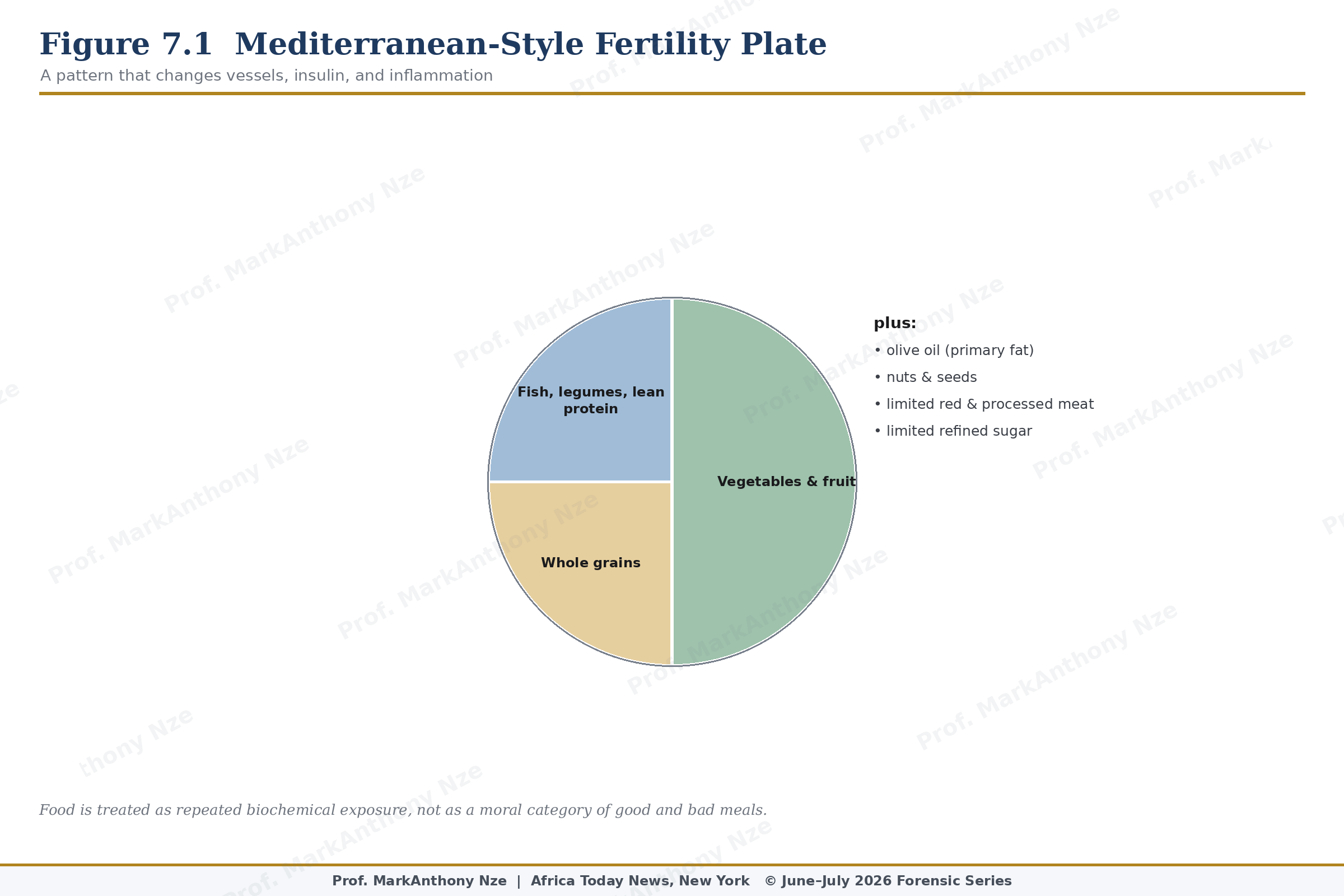
Figure 7.1. Mediterranean-Style Fertility Plate.
Protein adequacy is often under-discussed. Under-eating protein can impair satiety, muscle maintenance, glucose regulation, and recovery from exercise, while excessive reliance on refined carbohydrates can worsen glycemic swings in susceptible patients. Eggs, fish, legumes, lean meats, dairy when tolerated, tofu, nuts, and seeds can all play roles depending on culture, access, cost, and medical condition. Fertility writing should not confuse expensive food with better food.
Fiber is a quiet intervention with broad reach. Beans, lentils, vegetables, fruit, oats, whole grains, nuts, and seeds slow glucose absorption, support gut microbial products, improve satiety, and can assist lipid control. Stable glucose matters because insulin strain can affect PCOS expression, abdominal fat, vascular health, and inflammatory tone. A plate that protects glucose is also protecting reproductive conditions in selected patients.
Read also: The Fertility Repair Series—Part 6
Fats require distinction rather than fear. Olive oil, nuts, seeds, oily fish, avocado, and other unsaturated fat sources can support cardiometabolic patterns, while heavy intake of trans fats and ultra-processed foods may worsen metabolic strain. Omega-3 intake has plausible value through inflammation and vascular effects, though claims should stay measured. A fertility plate is built around fat quality, not fat panic.
Hydration and sugar drinks belong in the audit because many couples ignore liquid calories. Sweetened beverages can add glucose load without satiety, while heavy alcohol can distort sleep, appetite, liver metabolism, sexual function, and judgment around timing. Water is not a fertility cure. It is the baseline that should not have to compete with daily sugar exposure.
Folate deserves a formal place because pregnancy begins before pregnancy is recognized. Persons who may become pregnant are advised to take folic acid in the periconceptional period to reduce neural tube defect risk. Food sources such as leafy greens, beans, citrus, and fortified grains help, but supplementation remains standard advice in many settings. This is one of the least glamorous and most defensible preconception interventions.