Exercise As Reproductive Medicine
Movement repairs circulation before it repairs confidence.
Exercise is often sold as body-shaping when its reproductive value is mostly vascular and metabolic. Walking, cycling, swimming, resistance training, and structured movement alter blood pressure, endothelial function, insulin sensitivity, inflammatory load, mood, body composition, and sleep quality. Those changes reach the bedroom and the ovary before any mirror becomes relevant.
Male erectile function benefits when circulation improves. Aerobic exercise has evidence for improving erectile scores in many men with ED, particularly when cardiometabolic risk is present. Better endothelial function means better nitric-oxide availability and arterial responsiveness. Improved fitness also lowers fatigue, supports mood, reduces abdominal fat, and can restore sexual confidence without pretending that exercise is a universal cure.
Resistance training deserves equal respect. Muscle is a glucose-disposal organ, and greater muscle mass can improve insulin handling, body composition, and metabolic resilience. Men with central adiposity, low fitness, insulin resistance, or low testosterone symptoms may benefit from progressive strength work. Women with PCOS or metabolic risk may also gain from resistance training because muscle changes the glucose economy.
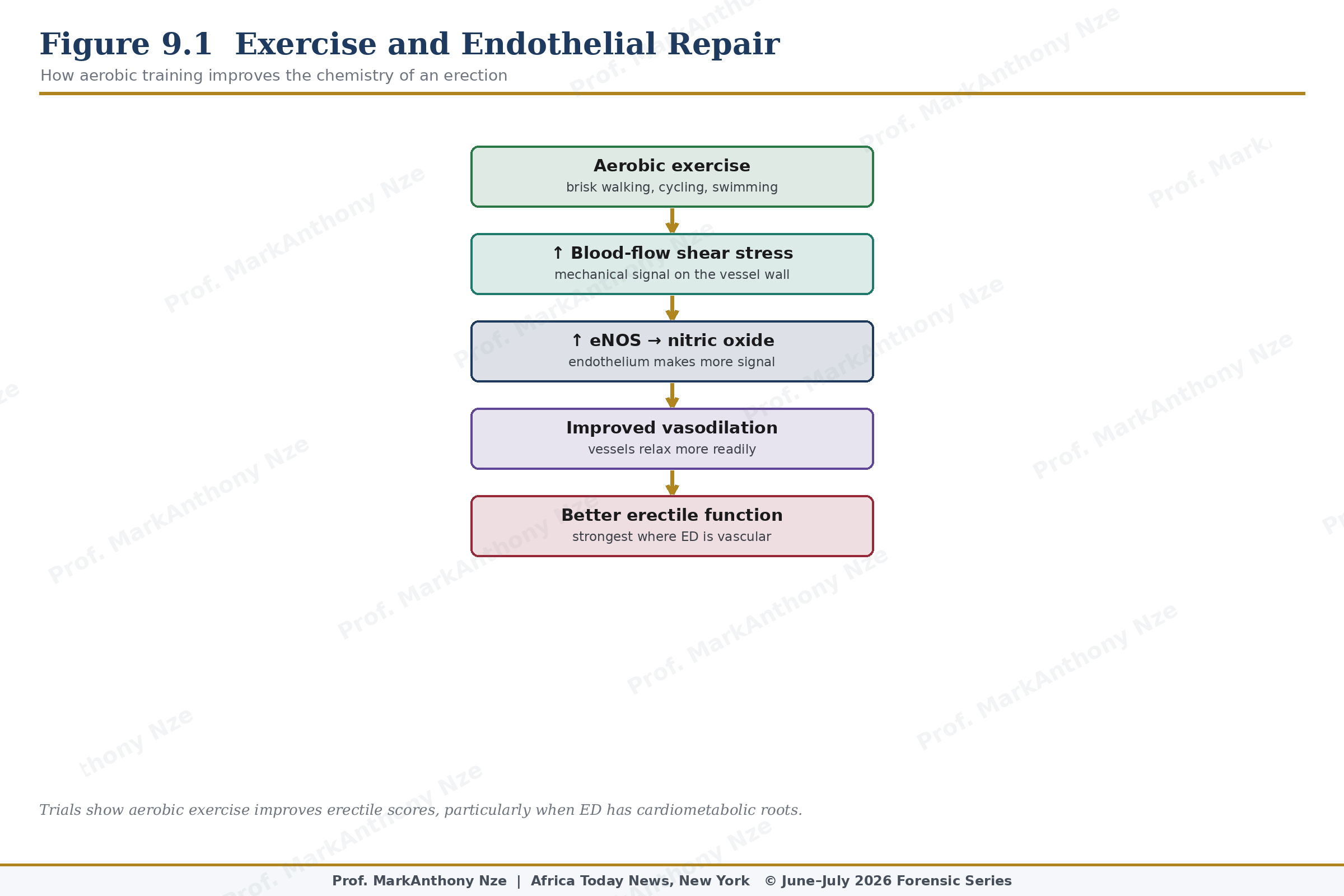
Figure 9.1. Exercise And Endothelial Repair.