The Male Partner Is Not A Footnote
A semen sample can prevent months of misdirected treatment.
Ejaculation is frequently mistaken for fertility proof. A man can produce semen while having low sperm concentration, poor motility, abnormal morphology, impaired vitality, obstruction, retrograde ejaculation, hormonal suppression, infection, varicocele-related heat stress, or sperm DNA injury. Visual confidence tells the couple almost nothing. Laboratory analysis is the opening document.
Current male-infertility guidance places semen analysis, reproductive history, physical examination, and assessment of behavioral or lifestyle risks inside the first diagnostic layer. WHO’s semen manual standardizes examination and processing because semen testing is method-sensitive and biologically variable. One abnormal result may need repeat testing. Avoiding the first result altogether is the larger failure.
A man’s reproductive history should be specific enough to feel inconvenient. Childhood undescended testis, mumps orchitis, testicular trauma, hernia repair, pelvic surgery, varicocele, vasectomy, chemotherapy, radiation, urinary infection, sexually transmitted infection, anabolic steroid exposure, testosterone therapy, opioid use, finasteride use, diabetes, hypertension, obesity, sleep apnea, smoking, cannabis, alcohol, pesticide exposure, solvent exposure, heat exposure, and erectile or ejaculatory problems all belong in the file.
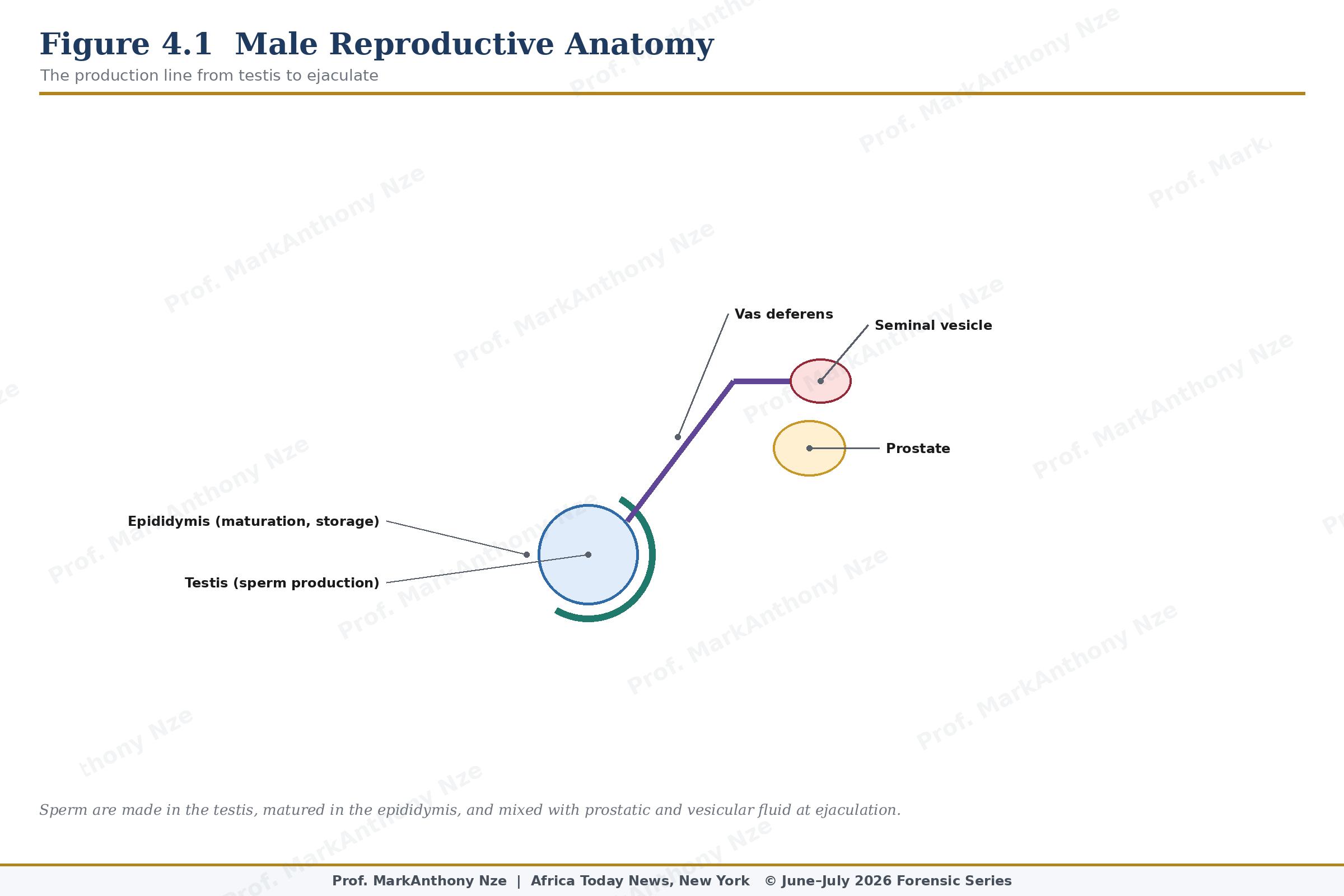
Figure 4.1. Male Reproductive Anatomy.
Male fertility also changes over time, though not with the same public attention given to female age. Advancing paternal age can affect semen parameters, sperm DNA integrity, miscarriage risk, and some offspring outcomes, with evidence varying by endpoint. That does not mean older men cannot father children. It means paternal age belongs in counseling instead of being hidden behind female age alone.
Testosterone deserves separate suspicion. Men often associate testosterone with virility, strength, libido, and erection quality, but exogenous testosterone can suppress luteinizing hormone and follicle-stimulating hormone, lowering intratesticular testosterone and impairing spermatogenesis. A man using testosterone or anabolic steroids may look more muscular while his semen quality deteriorates. Fertility goals must be discussed before hormonal treatment, not after damage becomes visible.
Read also: The Fertility Repair Series—Part 3
Varicocele is another frequent blind spot. Dilated veins around the testicle can raise local temperature, alter testicular environment, and contribute to abnormal semen parameters in selected men. Not every varicocele requires treatment, and not every semen abnormality is caused by varicocele. Physical examination by a trained clinician matters because a self-diagnosed scrotal problem and a clinically meaningful varicocele are not the same event.
Heat exposure belongs in ordinary counseling because sperm production is temperature-sensitive. Regular hot baths, frequent sauna use, occupational heat, laptop heat, tight heat-retaining clothing, and prolonged sitting may matter in some men, particularly when other risks are present. Heat reduction is not miracle treatment. It is exposure control. Within a 90-day audit, it becomes one measurable intervention among several.
Lifestyle risk should be discussed without moral theater. Smoking is linked with reduced semen quality and vascular injury. Heavy alcohol use can affect hormones, libido, semen parameters, liver function, sleep, and relationship behavior. Obesity can worsen insulin resistance, inflammation, testosterone balance, and scrotal thermal environment. Poor sleep may alter reproductive hormones and semen quality. These risks do not mean every exposed man is infertile, but they create modifiable pressure.
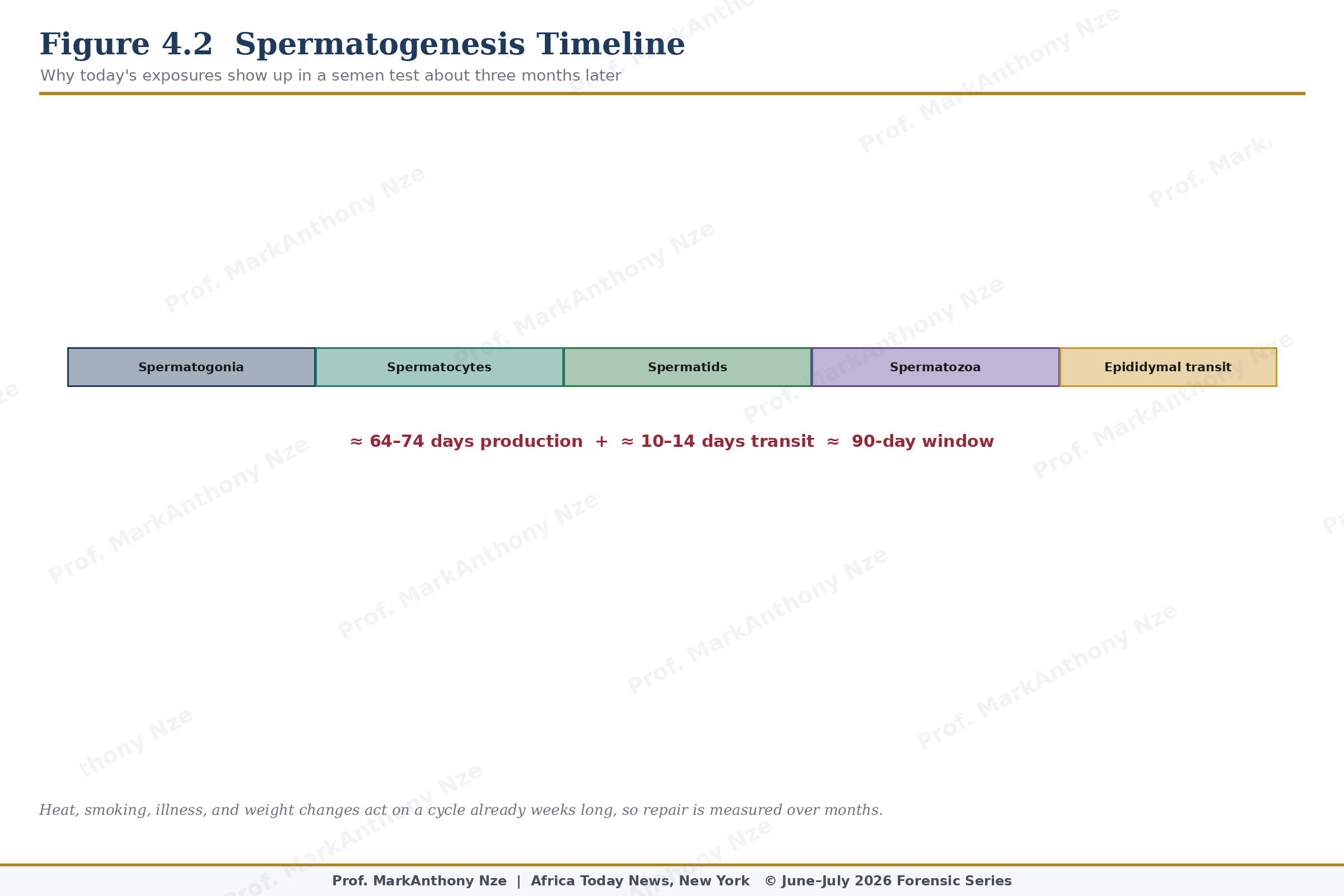
Figure 4.2. Spermatogenesis Timeline.
Occupational and environmental exposure cannot be dismissed as fringe concern. Pesticides, solvents, heavy metals, endocrine-disrupting chemicals, heat, radiation exposure, and industrial agents may affect semen parameters depending on dose, duration, protection, and individual susceptibility. Farm exposure, factory work, painting, welding, dry cleaning, chemical handling, frequent heat, military exposure, and poor ventilation deserve attention. Protective equipment is reproductive medicine in plain clothes.
Erectile and ejaculatory dysfunction sit directly inside fertility. A man may produce adequate sperm and still fail to deposit semen during the fertile window. Delayed ejaculation, premature ejaculation, retrograde ejaculation, anejaculation, painful ejaculation, and performance anxiety can all reduce conception probability. Fertility writing that treats sex mechanics as separate from reproduction avoids the room where reproduction is supposed to occur.
Infection deserves a careful file. Past epididymitis, prostatitis-like symptoms, sexually transmitted infections, urinary infections, painful ejaculation, pelvic pain, and leukocytes in semen may point toward inflammation or infection requiring medical review. Antibiotics should not be taken casually, but infection cannot be wished away by heat avoidance or vitamins. Laboratory evidence must decide.
Read also: The Fertility Repair Series — Volume I Overview
Semen analysis should be explained rather than feared. Concentration measures sperm per milliliter. Total count reflects volume multiplied by concentration. Motility measures movement, with progressive motility especially relevant. Morphology evaluates shape under strict criteria. Volume may point toward collection problems, ejaculatory duct issues, androgen status, or accessory gland function. Leukocytes may suggest inflammation or infection. No single number defines the whole man.
Repeat testing protects against overinterpretation. Fever, viral illness, recent heat exposure, abstinence interval, collection loss, lab handling, and medication changes can alter results. Sperm production reflects prior weeks and months, not just the day of collection. A 90-day intervention period may be useful when modifiable risks exist, but severe abnormalities require specialist referral rather than endless lifestyle loops.
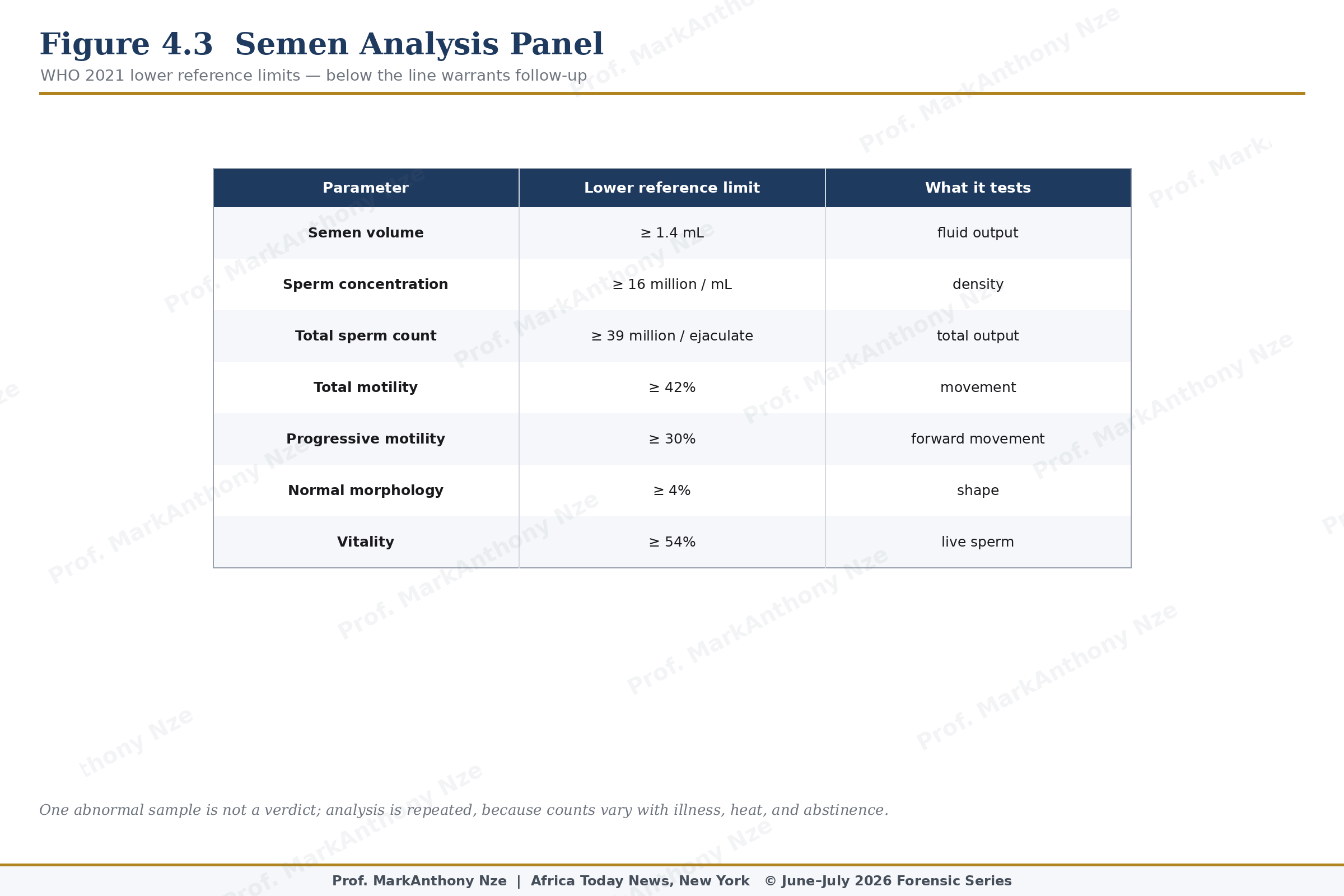
Figure 4.3. Semen Analysis Panel.
Genetic causes are not common in every man, but severe oligozoospermia or azoospermia may require genetic testing. Y-chromosome microdeletions, karyotype abnormalities, or congenital absence of the vas deferens can change treatment, prognosis, and family counseling. Natural remedies have no authority over missing genes or absent ducts. Pretending otherwise converts hope into fraud.
Male infertility also carries broader health meaning. AUA/ASRM guidance notes that abnormal sperm production can be associated with health risks, which is why male infertility should not be treated only as a couple’s pregnancy obstacle. Testicular dysfunction, endocrine disease, genetic conditions, malignancy risk, metabolic disease, or systemic illness may appear through fertility testing. Semen analysis may become a health door the man never expected to open.
Cultural resistance is predictable. Some men interpret testing as accusation, weakness, or attack on masculinity. Some families protect male pride while interrogating the woman. Some communities still treat infertility as female failure until a laboratory proves otherwise, and even then silence may continue. Medical truth has to be louder than inherited blame. Couples lose time when male testing is delayed for social comfort.
A semen sample is not a verdict on manhood. It is a biological specimen produced by an organ system exposed to hormones, heat, toxins, disease, medication, sleep, stress, age, and blood supply. Treating it as shameful protects ignorance. Testing it protects the couple.
A couple’s fastest path may begin with the simplest male test. Before months of female-only investigation, before expensive supplements, before accusation, before another cycle is lost, semen must be seen. Anything less allows culture to outrank biology.
Every infertility conversation should therefore carry one practical demand: test both partners early. A man who agrees to evaluation is not surrendering pride; he is sharing the burden of evidence.
Female partners also need protection from the hidden cost of male delay. Every month spent avoiding semen analysis may become another month of invasive female testing, family accusation, and age-related loss. A serious man does not protect pride by avoiding the laboratory. He protects his household by submitting evidence early.
Sperm quality should also be linked to general health in language men understand. Poor semen findings may sit beside diabetes, obesity, hormonal disease, testicular problems, genetic risk, or occupational exposure. A man who learns this early may gain more than fertility information. He may find the first evidence of a neglected health problem.
Testing early also protects money. Couples may spend heavily on supplements, scans, spiritual consultations, and repeated female-only visits while the male result remains unknown. A semen analysis is often less costly than months of delay. Refusal can be expensive.
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.