
Belly Fat, Insulin And Bedroom Failure
Central adiposity is not cosmetic; it is endocrine interference.
Belly fat is often discussed with the wrong vocabulary. Beauty language misses the medical event. Visceral adipose tissue behaves like endocrine and inflammatory tissue, influencing insulin resistance, vascular function, testosterone balance, ovulatory pattern, sleep apnea risk, blood pressure, lipid metabolism, and chronic inflammation. When reproduction fails in the presence of central adiposity, the waist is not a side issue.
Insulin resistance sits near the center of this file. Cells respond poorly to insulin, the pancreas produces more, glucose control becomes unstable, and downstream hormonal effects appear. In men, insulin resistance travels with endothelial dysfunction, low testosterone in some cases, abdominal fat, hypertension, and ED. In women, especially those with PCOS, insulin excess can amplify androgen production and disrupt ovulation.
PCOS makes the metabolic-reproductive link visible. Irregular cycles, acne, hirsutism, weight gain, central adiposity, insulin resistance, sleep apnea risk, and difficulty conceiving may appear together. Not every woman with PCOS has obesity, and not every woman with obesity has PCOS. Still, when insulin resistance is present, lifestyle repair becomes more than weight talk. It becomes ovulation strategy.
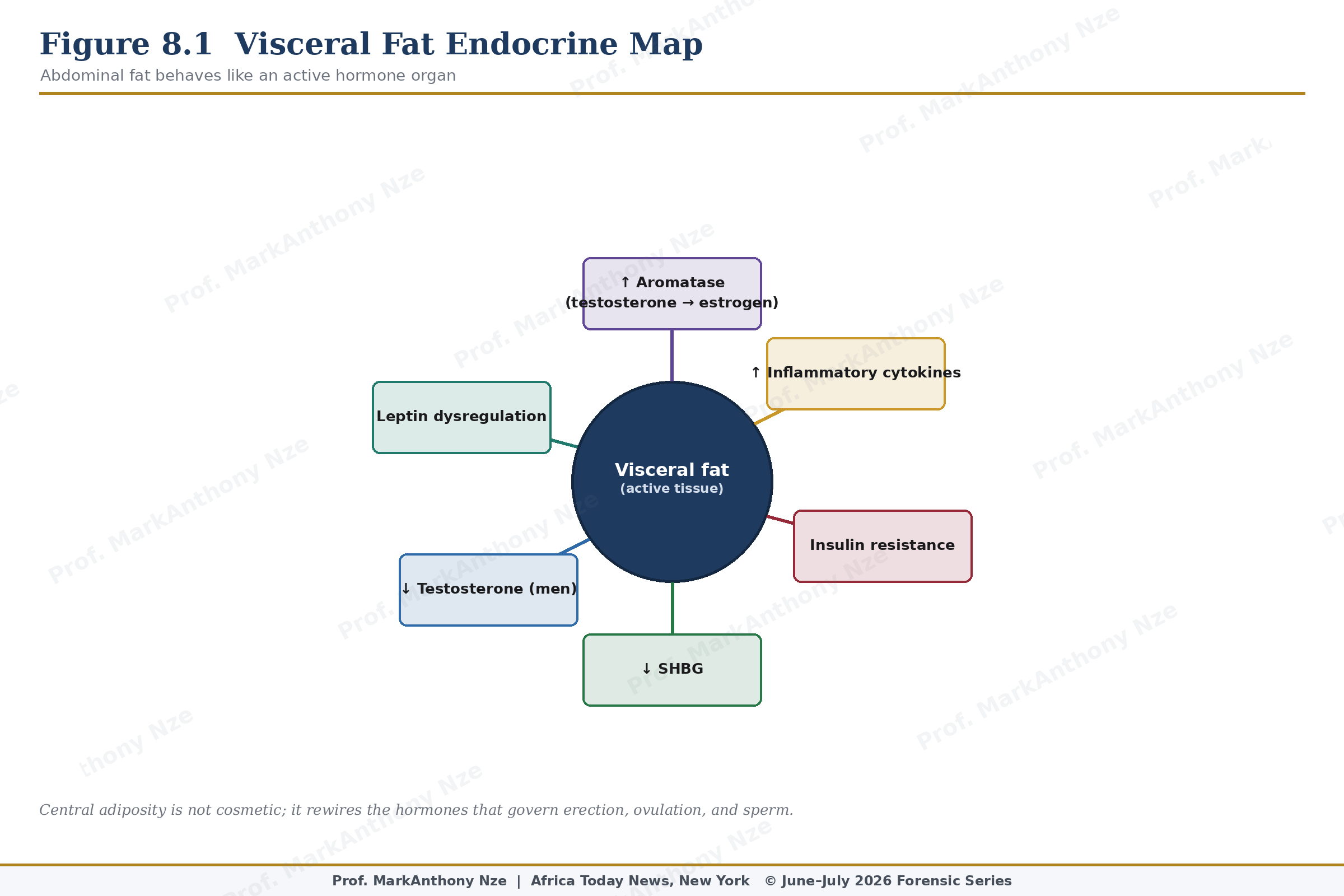
Figure 8.1. Visceral Fat Endocrine Map.
Male sexual function also bends under metabolic load. Visceral fat can worsen endothelial function, reduce nitric oxide availability, increase inflammation, and lower testosterone in selected men. Sleep apnea often rides along, adding oxygen disruption and fatigue. Diabetes risk rises. Blood pressure follows. A man may experience ED before he calls himself sick because the penile vascular bed has less tolerance for metabolic negligence.
Weight advice must be handled without contempt. Shame does not improve insulin sensitivity. Humiliation does not restore ovulation. A patient who feels attacked may avoid care, binge in secrecy, stop exercising, or buy fraudulent products promising rapid transformation. Clinical writing should be unsentimental about risk and humane about the person carrying it.
Inflammation provides the bridge between appearance and disease. Visceral fat can produce cytokine signals that affect vascular function, insulin response, liver metabolism, and ovarian physiology. Reproductive organs are not sealed away from this chemistry. Sperm production, penile blood flow, follicular development, and endometrial readiness all occur inside the same body-wide metabolic weather.
Read also: The Fertility Repair Series—Part 7
Waist circumference deserves measurement because scale weight can deceive. Two people with similar weight may carry very different metabolic risk depending on muscle mass, fat distribution, activity, ethnicity, and medical history. Central adiposity is more strongly tied to insulin resistance than cosmetic appearance suggests. Measuring the waist converts a vague impression into a trackable marker.
Natural repair begins with muscle and glucose. Resistance training increases muscle mass and improves glucose disposal. Aerobic movement improves insulin sensitivity, endothelial function, blood pressure, and mood. Protein adequacy improves satiety and supports muscle. Fiber slows glucose absorption. Sleep repair reduces appetite dysregulation and sympathetic stress. None of these steps requires a miracle product.