Pelvic Pain, Painful Sex And Female Fertility
Pain during sex is evidence, not temperament.
For years a woman is told that sex hurts because she is tense, or inexperienced, or anxious, or simply too sensitive. She learns to brace, to apologize, to get through it. Then the couple starts trying for a baby, and the pain she was taught to ignore suddenly becomes the thing standing between them and a pregnancy. Only now does anyone treat it as information. Pain with penetration, deep pelvic pain, burning, tearing, aching afterward, agony during menstruation: these are not features of a personality. They are clinical data that were dismissed the first several times they were reported.
Painful sex interrupts conception through more than one route at once. Intercourse gets avoided, cut short, or mistimed, and each guarded attempt tightens the muscles for the next one. A couple misses the fertile window because sex has quietly become a threat. A woman stops mentioning the pain because mentioning it produces blame instead of help. Months slide past, the problem gets filed as bad timing, and the pelvis keeps signaling a disease that no one is listening to.
Endometriosis sits near the top of the list of suspects, especially when the pain follows the cycle, with severe cramps, deep pain during sex, bowel or bladder symptoms around bleeding, and fatigue. Guidance from ESHRE treats it as a disease that deserves structured diagnosis and management for both pain and infertility, not as dramatic menstruation to be waited out (Becker et al., 2022). The disease is also inconsistent: some women have severe symptoms, others have surprisingly little pain and still face infertility, and a quiet history does not rule it out.
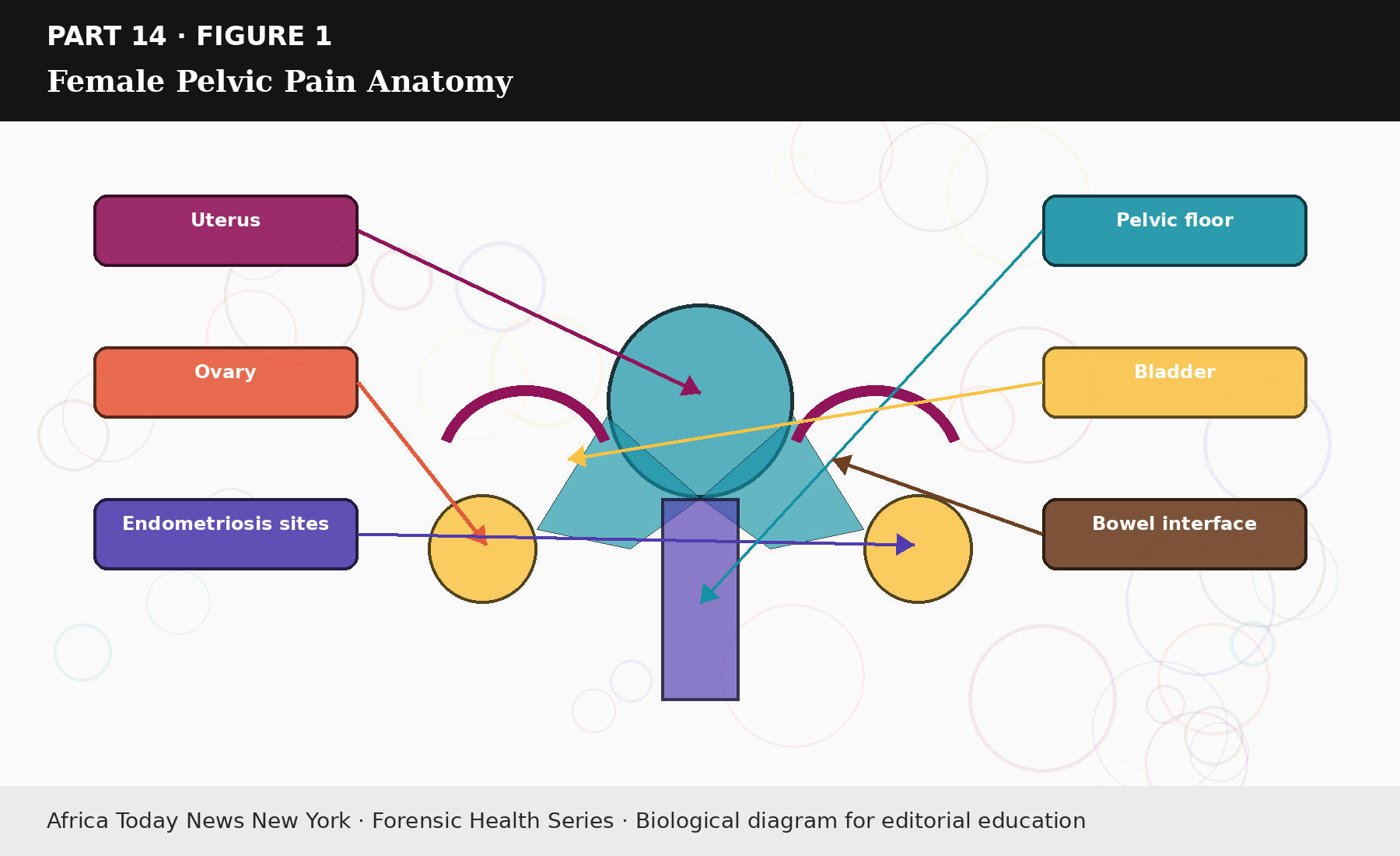
Figure 14.1: Female Pelvic Pain Anatomy.
Pelvic-floor dysfunction can exist with endometriosis or entirely without it. Muscles learn to guard after repeated pain, after trauma, after a difficult birth, an infection, surgery, or long inflammation, and once the guarding is learned, penetration can trigger a clench before the couple has time to understand what happened. Lubricant helps with dryness, but it does nothing for a floor that spasms, a vulva carrying nerve pain, or lesions dragging on tissue. The list of possibilities is longer still: vaginismus, vulvodynia, hormonal thinning, recurrent infection, skin disease, bladder pain syndrome, irritable bowel patterns, ovarian cysts, fibroids, adhesions, and old surgical scarring can each take a seat in the file.
Read more…
Read also: The Fertility Repair Series—Part 13
This is why the standard fertility instruction to “have sex every other day” is careless when nobody has asked whether sex hurts. A schedule laid down over untreated pain becomes coercive even in a loving marriage, and it teaches the body to defend itself harder each cycle. Physical therapy has a real place, but only once the problem has an accurate name. Pelvic-floor therapy can include education, external and internal assessment, relaxation training, manual work, graded exposure, breathing, dilators when appropriate, and scar management, with strengthening saved for later if it is needed at all. Reviews of pelvic-floor treatment for painful sex and sexual dysfunction report meaningful benefit, while noting that the evidence quality varies and that patient selection matters (Fernández-Pérez et al., 2023; Jorge et al., 2024). Therapy is a genuine tool, not a substitute for imaging, infection treatment, or specialist care.
Referral should not wait when the pain is severe or getting worse, when it comes with abnormal bleeding, fever, foul discharge, a new pelvic mass, or a history of pelvic infection, or when there is infertility, recurrent miscarriage, or an inability to tolerate an exam. Women are trained to endure reproductive pain, sometimes for a decade, and by the time they finally ask for help the condition has often reshaped sex, mood, marriage, and reproductive timing all at once.
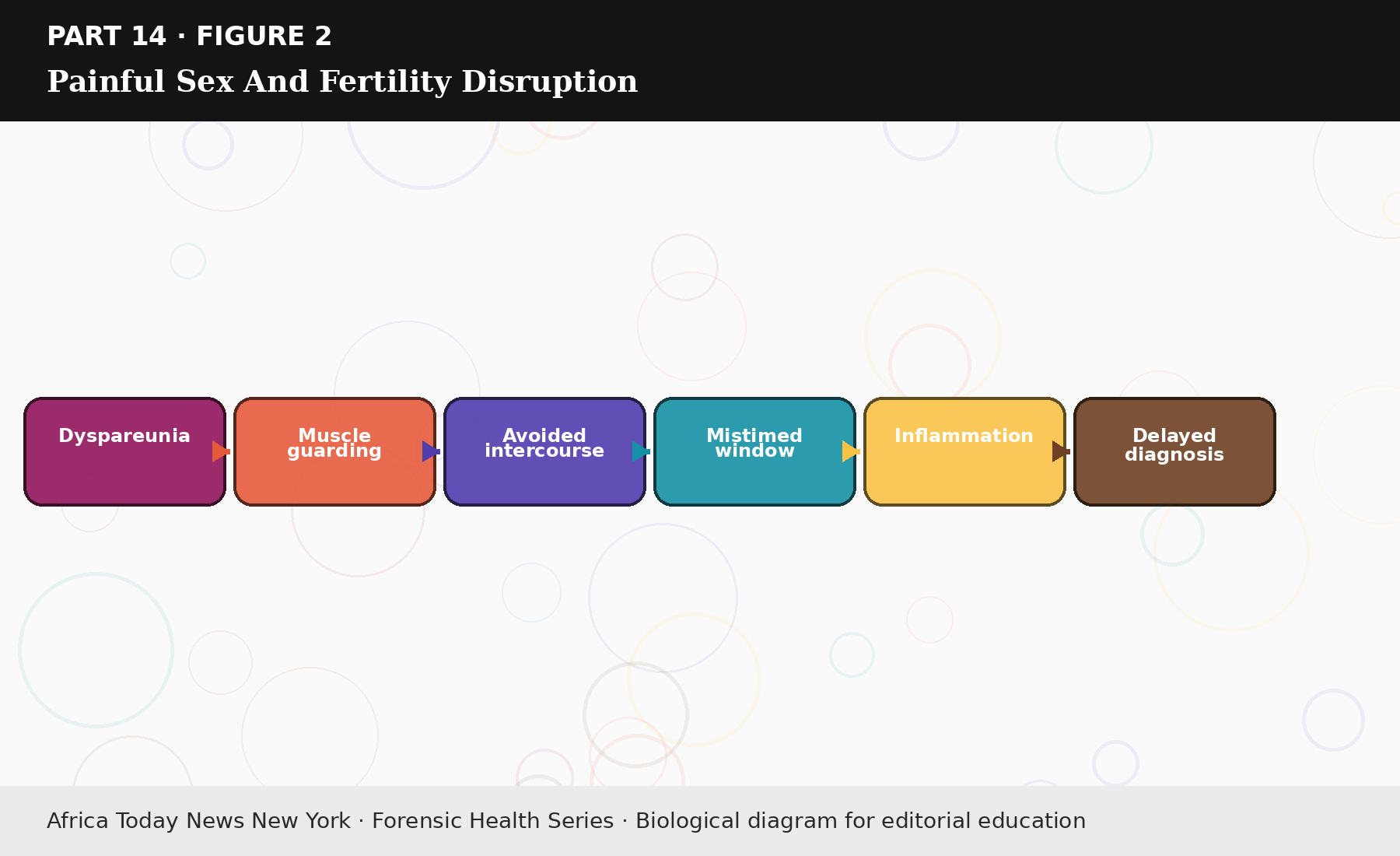
Figure 14.2: Painful Sex And Fertility Disruption.
Natural support has a role while the diagnosis is worked out, provided nobody oversells it. Better sleep, an anti-inflammatory pattern of eating, treatment of constipation, heat, gentle movement, less alcohol, and careful tracking of cycle-linked symptoms can help some women function more comfortably. None of that should be used to tell a woman with disabling pain that she can lifestyle her way past an evaluation. Comfort measures support the work; they do not replace it, and a quieter pelvis can still hide endometriosis, adhesions, fibroids, or a sensitized nerve.
Sexual repair has to be built around consent. Penetration should not be the only measure of intimacy during a painful stretch, and couples often need non-penetrative sex, agreed stopping points, better lubrication, pain treatment, and a fertility plan that does not turn the woman’s body into a timed instrument. Intercourse for conception should never require her to dissociate from what she is feeling. Culture makes this harder than it needs to be: some communities treat painful sex as a wife’s duty to push through, some warn that discussing pelvic symptoms is indecent, and some partners read refusal as rebellion. Each of those beliefs delays care and turns pain into private property.
Read also: The Fertility Repair Series—Part 12
Clinicians add to the injury when they wave off severe period pain or rush through a pelvic exam that leaves a woman more frightened than before. A patient who has been dismissed tends to avoid the next visit, and then gets blamed for a late diagnosis that the system helped produce. Trust has to be rebuilt deliberately, through explanation, consent, trauma-aware pacing, and a plan that respects both the pain and the goal of pregnancy. A rushed exam or a forced speculum is remembered, and it makes the next appointment less likely to happen at all.
Bladder and bowel symptoms should not be split off from pelvic pain too early. Urgency, burning without a proven infection, constipation, diarrhea flares, pain with bowel movements, and rectal pressure can travel with endometriosis, pelvic-floor dysfunction, bladder pain syndrome, or adhesions. Women tend to report these to different clinicians, and the file fragments across specialties; fertility care needs the whole pelvis described on one page rather than scattered across three.
Pain control itself has to respect the fertility goal, which is where sequencing becomes medicine rather than contradiction. Anti-inflammatory drugs, hormonal suppression, surgery, pelvic therapy, neuropathic pain treatment, or assisted reproduction may each be reasonable depending on the diagnosis and on whether the couple is actively trying now. A treatment that relieves pain may also postpone pregnancy for a time, and saying so honestly lets a woman choose the order that fits her situation instead of being handed a single script.
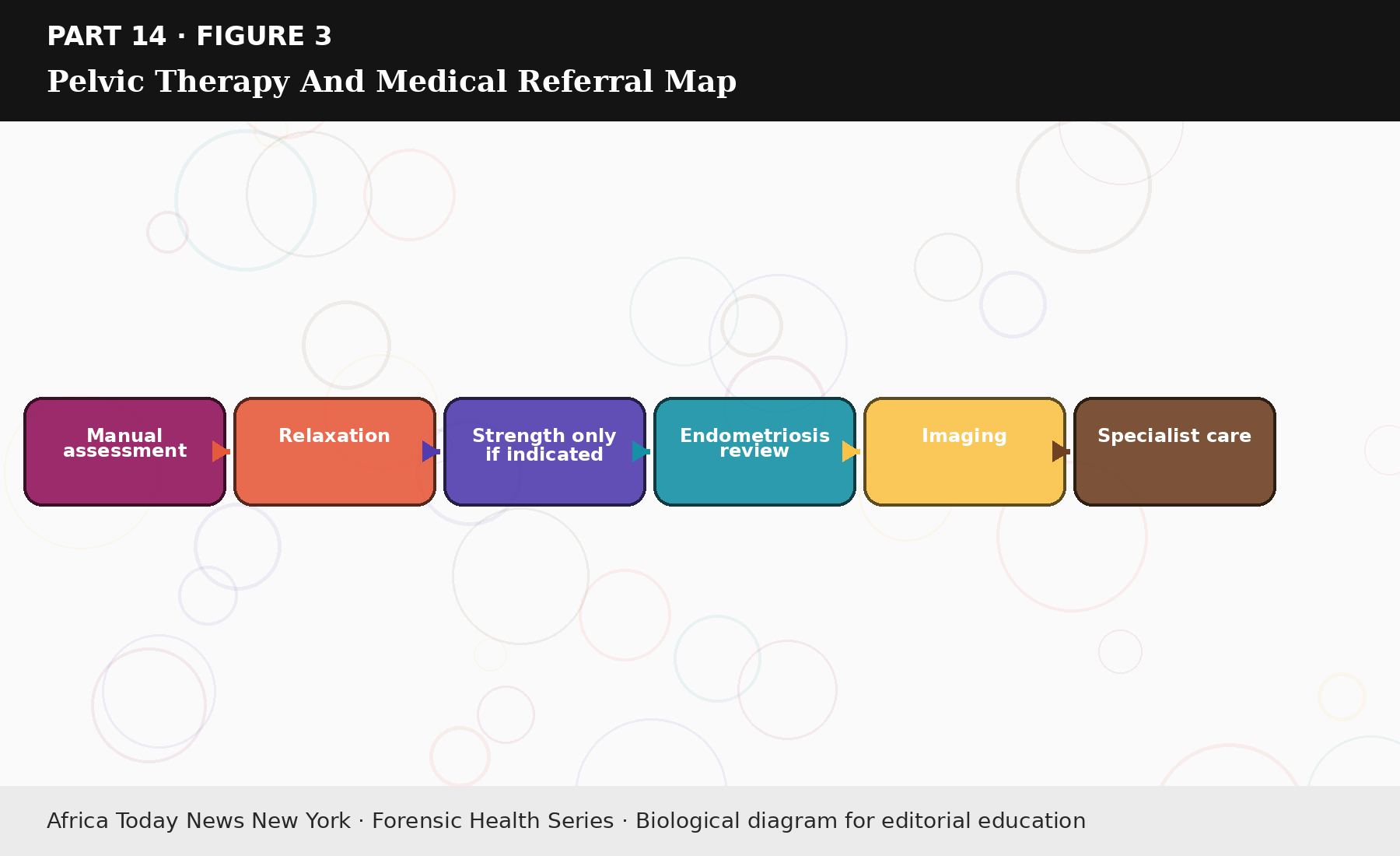
Figure 14.3: Pelvic Therapy And Medical Referral Map.
Fertility timing can bend around all of this rather than override it. Ovulation tracking can cut down on unnecessary attempts, semen analysis can spare wasted cycles if the male factor is present, lubricant can be reviewed, pelvic therapy can ease the guarding, and endometriosis or cavity disease can be investigated in parallel. A pain diary that records bleeding, bowel and bladder symptoms, pain with sex, ovulation pain, and spotting turns a vague complaint into a pattern that is much harder to dismiss. Male partners carry real obligations inside female pain: demanding intercourse through it is not support but further harm, while attending appointments, accepting non-penetrative intimacy, and completing a semen analysis are. Pain is one of the body’s few honest witnesses, and ignoring it because a pregnancy is wanted does not honor fertility so much as sacrifice the patient to a calendar.
Source & Clinical Standards
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.