PCOS, Insulin Resistance And Natural Ovulation Support
PCOS is not an ovarian problem alone.
PCOS is usually explained as cysts on the ovaries, which is where the confusion starts. Plenty of women with the condition have no dramatic cyst story at all. What they have is some combination of irregular cycles, excess androgen, acne or unwanted hair, stubborn weight, insulin resistance, infertility, low mood, poor sleep, and long-term metabolic risk, none of which was ever gathered into a single diagnosis. The look of the ovary on a scan can matter, but the disorder is not a photograph. It is a reproductive-metabolic pattern that plays out across the whole body.
Insulin resistance sits at the center of that pattern for many women. When cells resist insulin, the pancreas answers with more of it, and that high-insulin environment can push the ovary toward more androgen, disturb the growth of follicles, and scatter ovulation. Weight gain can deepen the resistance, but lean women get PCOS too, so reducing the condition to body size is both inaccurate and unkind. Metabolism is not the same thing as the number on a scale, and treating it as though it were sends a lot of women away feeling blamed for a problem they did not cause.
Read also: The Fertility Repair Series—Part 14
Current international guidance treats PCOS across three domains at once, reproductive, metabolic, and psychological, with attention to diagnosis, lifestyle, cycles, androgen excess, fertility, and long-term health (Teede et al., 2023). That breadth matters, because women are so often handed fragmented care. A dermatologist treats the acne, a gynecologist prescribes a pill for the bleeding, a fertility clinic induces ovulation, and nobody sits down to explain the metabolic engine driving all of it.
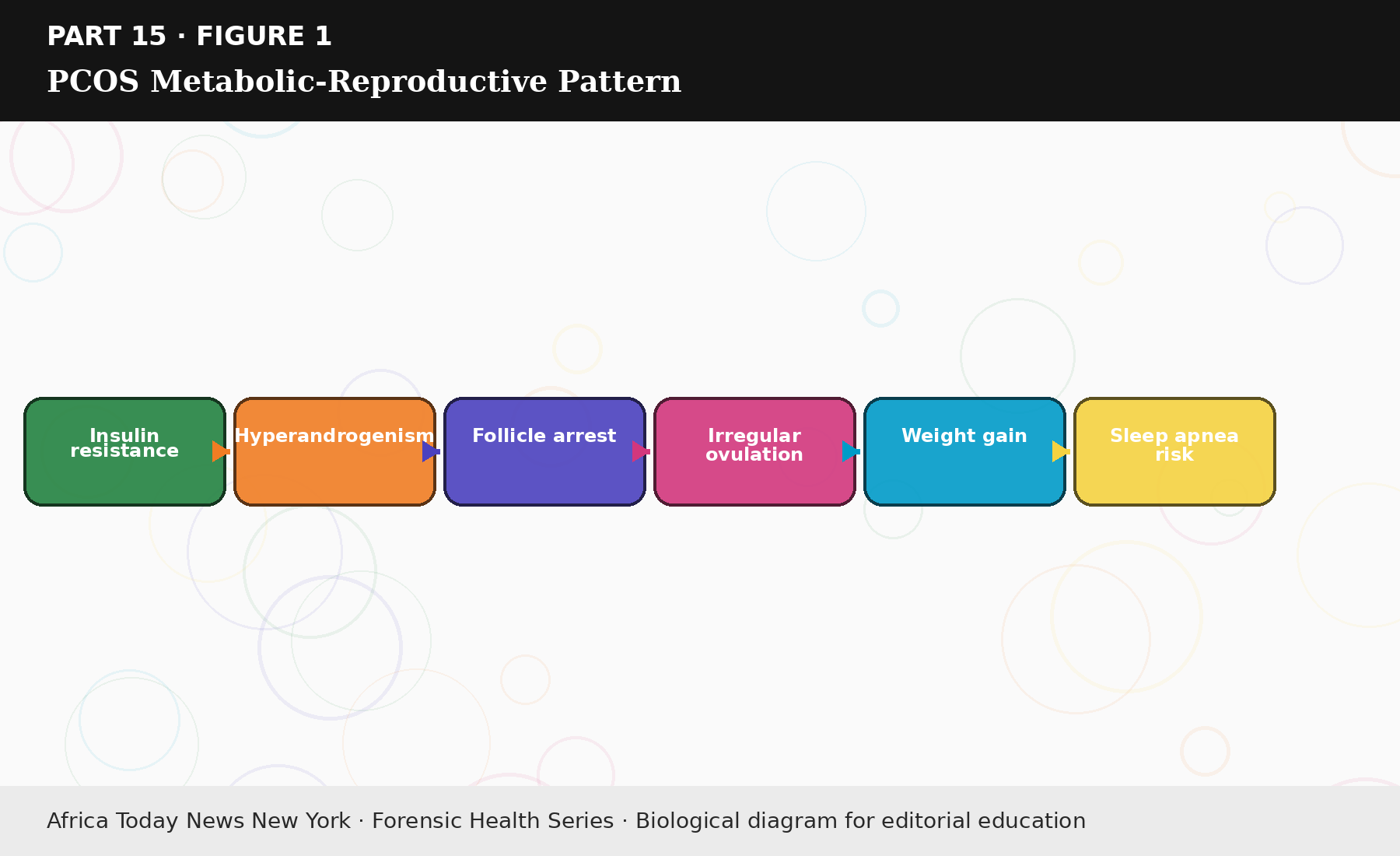
Figure 15.1: PCOS Metabolic-Reproductive Pattern.
Read more…