
Erectile Dysfunction As A Vascular Warning From The Body
The penis is often the first artery to confess.
New erectile dysfunction should be treated as a vascular message until evidence proves otherwise. Desire may remain intact while arteries fail, nerves misfire, smooth muscle resists relaxation, venous trapping weakens, or medication suppresses sexual response. Embarrassment focuses attention on performance, but performance is only the visible endpoint of a sequence that begins in the vascular lining and nervous system.
Penile erection depends on endothelial competence. Sexual stimulation triggers neural release of nitric oxide and related signals, allowing cavernosal smooth muscle to relax and blood to fill the corpora cavernosa. As erectile tissue expands, venous channels are compressed against the tunica albuginea so rigidity can persist. Damage this pathway and the erection becomes soft, brief, unreliable, or absent.
Small arteries make the penis a ruthless reporter. Penile vessels are narrower than many coronary vessels, so vascular injury may become sexually visible before chest pain, breathlessness, or a diagnosed heart event. Princeton IV consensus work places ED inside cardiovascular risk thinking because erectile failure may identify men who need cardiometabolic evaluation rather than mockery, secrecy, or unregulated capsules.
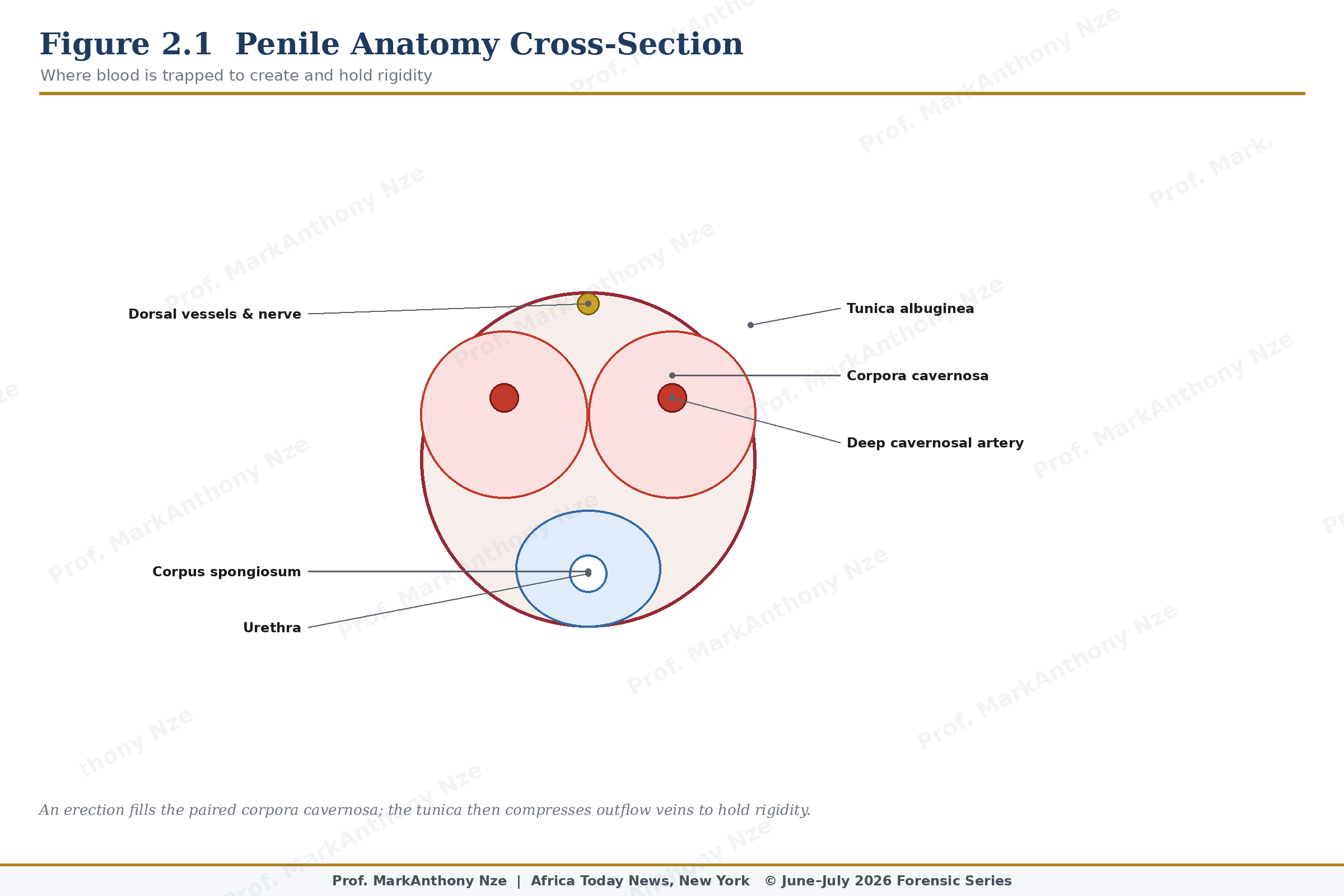
Figure 2.1. Penile Anatomy Cross-Section.
Diabetes provides a clean example because it injures erection through several routes at once. Hyperglycemia damages endothelial function, contributes to neuropathy, raises oxidative stress, alters smooth-muscle behavior, and travels with kidney disease, hypertension, obesity, dyslipidemia, and depression. A man with diabetes and ED is not facing a bedroom inconvenience alone. His sexual symptom may be tracking microvascular damage.
Cardiovascular review does not mean every man with ED is near a heart attack. It means the symptom deserves proportionate investigation: blood pressure, glucose status, lipids, waist, smoking, sleep, exercise tolerance, family history, medication profile, and chest symptoms. Men who appear healthy can still carry silent risk, and younger men with ED should not be dismissed because age flatters the chart.
Hypertension deserves equal attention because pressure injury stiffens vessels and impairs arterial responsiveness. Some blood-pressure medications may affect erection in selected patients, but self-discontinuation is dangerous. A man who stops treatment to preserve sex may expose himself to stroke, kidney injury, heart failure, or myocardial infarction. Medication review belongs with a clinician, not in a group chat.
Obesity alters erection through metabolic, hormonal, inflammatory, and mechanical routes. Visceral fat worsens insulin resistance, raises inflammatory signaling, lowers testosterone in some men, increases sleep-apnea risk, and usually travels with hypertension or lipid abnormality. Waist circumference may tell a sharper story than scale weight because abdominal fat behaves like endocrine tissue, not storage alone.
Sleep apnea must be asked about plainly. Loud snoring, witnessed pauses in breathing, morning headaches, daytime sleepiness, resistant hypertension, low libido, and central obesity can point toward a nightly oxygen problem. Poor oxygenation and sympathetic activation strain blood vessels, worsen insulin resistance, and disrupt testosterone rhythm. A man treating ED while ignoring severe sleep apnea is repairing the window while the roof leaks.
Read also: The Fertility Repair Series—Part 1
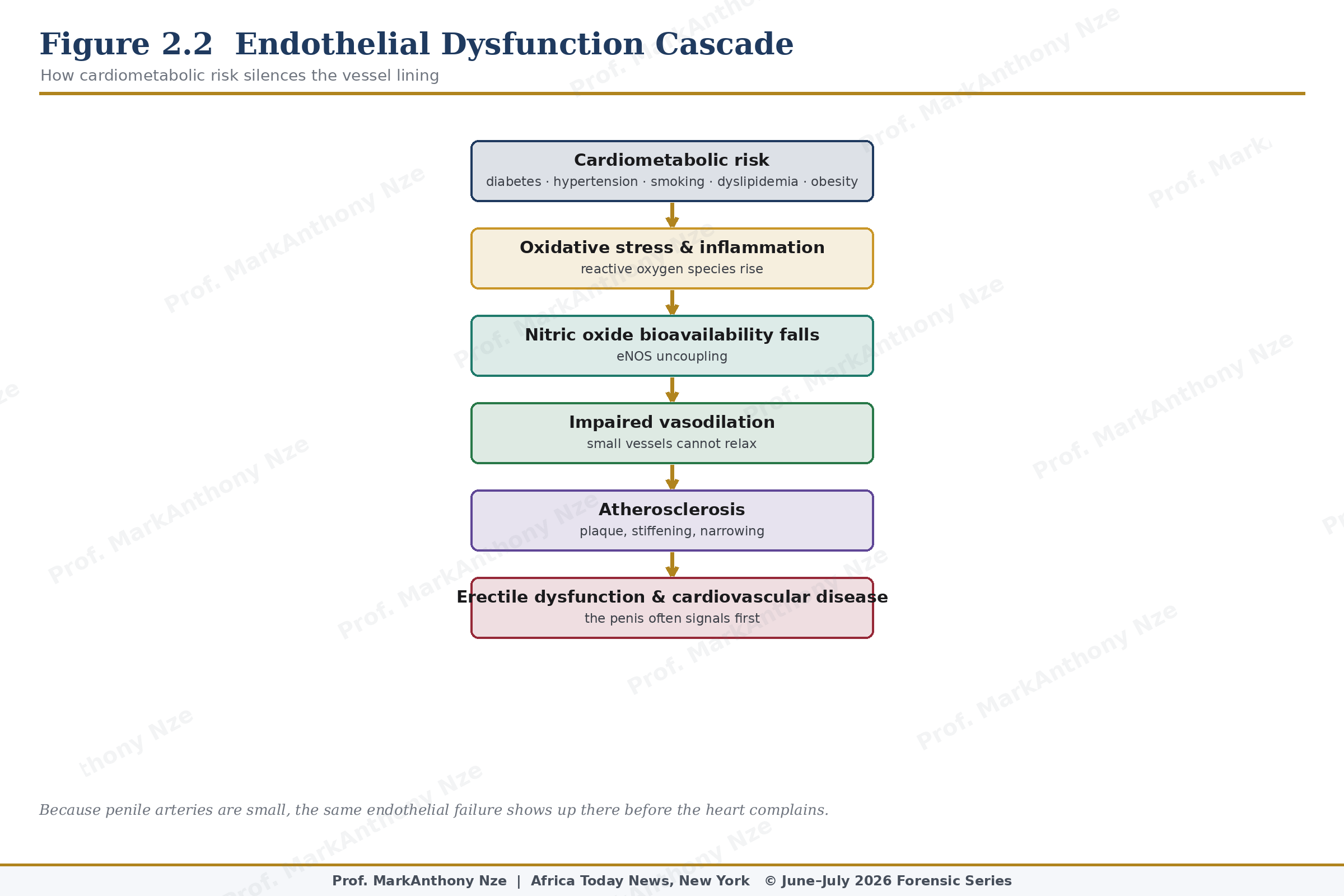
Figure 2.2. Endothelial Dysfunction Cascade.
Psychological factors do not make ED imaginary. Performance anxiety can activate sympathetic tone, narrow attention around failure, and interrupt erection even in men without severe vascular disease. Depression can reduce libido. Relationship injury can produce avoidance. Trauma can distort arousal and safety. Clean categories may please textbook writers, but patients usually arrive with mixtures.
Morning erections deserve attention because they reduce the noise of sexual context. Loss of nocturnal or early-morning erections often points toward organic contribution, while preserved spontaneous erections may suggest a stronger psychogenic or situational element. That distinction is not absolute, but it helps organize the file. Sexual medicine improves when pattern is respected.
Hormonal testing should be precise rather than theatrical. Low testosterone may appear with reduced libido, fewer morning erections, fatigue, low mood, muscle loss, increased fat mass, and poor erectile response. Casual testosterone use is dangerous for men trying to conceive because exogenous testosterone can suppress pituitary signaling and reduce sperm production. A man may feel sexually restored while fertility declines.
Pelvic floor dysfunction can also complicate the picture. Some men hold chronic tension through the pelvic muscles after pain, stress, urinary symptoms, prostatitis-like complaints, or sexual failure. Weakness and overactivity are different problems, and random Kegel exercises may worsen men who are already guarding. Pelvic physical therapy belongs in selected cases after assessment, not as a universal instruction.
Natural intervention for ED begins with circulation. Aerobic exercise improves endothelial function, blood pressure, insulin sensitivity, and erectile scores in many men, especially when ED has cardiometabolic roots. Resistance training improves muscle mass, glucose disposal, body composition, and metabolic resilience. A Mediterranean-style eating pattern may support vascular health through fiber, legumes, fish, nuts, vegetables, fruit, olive oil, and lower ultra-processed burden.
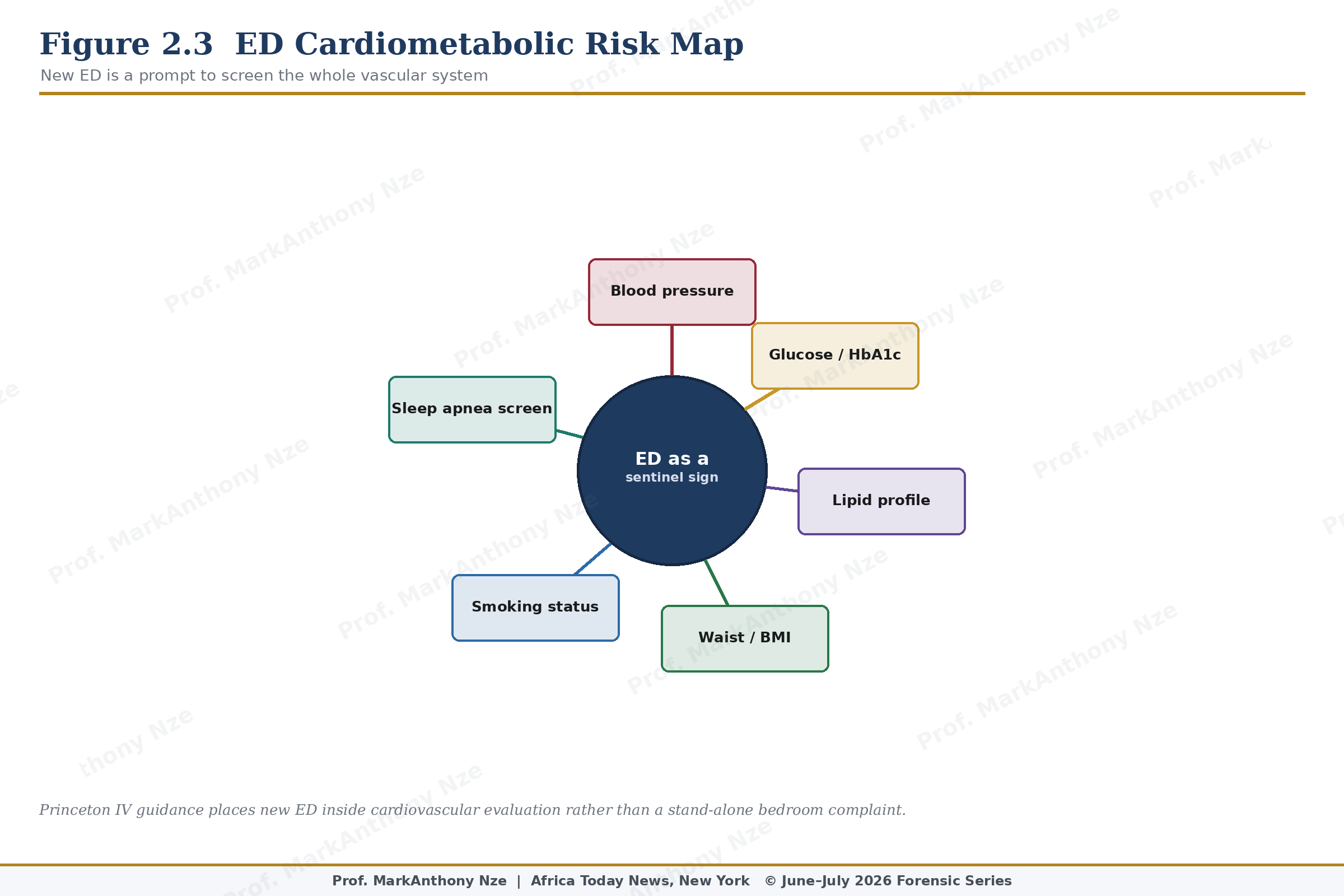
Figure 2.3. ED Cardiometabolic Risk Map.
Smoking cessation is not decorative advice. Tobacco damages blood vessels, increases oxidative stress, worsens nitric-oxide availability, and contributes to cardiovascular disease. Alcohol requires dose discipline because heavier intake can impair libido, testosterone, liver function, sleep quality, mood, and erection reliability. Cannabis and recreational substances deserve direct questioning because patients may not report exposure unless the question is asked without moral theater.
Prescription ED medication has a legitimate place, and moral panic over pills helps nobody. Properly prescribed PDE5 inhibitors have allowed many men to regain sexual function and relationship confidence. Medical supervision matters because contraindications, cardiovascular risk, nitrate use, blood-pressure instability, retinal issues, medication interactions, and treatment failure require judgment. Pharmacy medicine and gas-station medicine are not the same species.
Supplement caution should be severe. A bottle promising stamina may contain unknown doses, stimulants, contaminated ingredients, hormone-active compounds, or undeclared prescription drugs. Sildenafil and tadalafil are legitimate medications when prescribed and supervised. Hidden use is different. Nitrate interaction can be dangerous, cardiovascular disease can be missed, and a forced erection may be mistaken for recovery while the vascular problem remains unmeasured.
Practical ED assessment begins with pattern. Gradual loss of rigidity, reduced morning erections, diabetes, hypertension, smoking, dyslipidemia, obesity, or low exercise tolerance points toward organic contribution. Sudden situational failure with preserved morning erections may suggest anxiety, conflict, stress, or context. Pain, penile curvature, urinary symptoms, pelvic pain, testicular changes, medication shifts, neurologic symptoms, or ejaculation problems change the investigation. New ED with chest symptoms demands urgent medical review.
Men deserve blunt protection, not jokes. Erectile dysfunction may be the earliest socially visible sign of systemic vascular injury, and ignoring that possibility because the topic is embarrassing is bad medicine. Selling contaminated capsules into that fear is worse.
A natural ED plan should therefore read like a vascular rehabilitation plan with sexual consequences. Walk, lift, sleep, stop smoking, reduce alcohol, test glucose, review medications, measure pressure, correct weight when needed, investigate testosterone only with indications, and seek cardiovascular review when risk is present. A man who does that has not abandoned masculinity. He has stopped treating the penis as if it were detached from the rest of the body.
Bedroom silence is expensive. Every untreated year can deepen vascular risk, relationship strain, avoidance, and dependency on unsafe products. Early investigation protects health before the symptom hardens into identity.
Clinical documentation should include duration, severity, erection rigidity, masturbation response, morning erections, partner context, ejaculation, orgasm, pain, curvature, urinary symptoms, and libido. That detail prevents lazy classification. ED after a new medication, after pelvic surgery, after weight gain, after bereavement, or after diabetes progression is not the same story. Pattern is part of diagnosis.
Source & Clinical Standards
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.