
The 90-Day Fertility Audit
Ninety days is long enough to expose patterns and too short to excuse neglect.
Ninety days is not a miracle interval. It is a disciplined observation window long enough to expose behavior, physiology, and avoidance. Sperm development reflects weeks of prior testicular conditions. Exercise adaptation, sleep repair, alcohol reduction, glucose improvement, and dietary consistency need time. Cycle tracking needs more than one bleeding date. A couple that uses ninety days well may learn more than another couple learns in a year of guessing.
Audit language matters because it removes moral heat. A man is not asked to evaluate his own strength; the intake tracks the presence of morning erections, notes if erectile dysfunction is situational or progressive, and logs obstructive snoring or nicotine use. The clinical record requires known blood pressure trends, verified glucose metrics, any history of exogenous testosterone use, the mechanical capacity to ejaculate during the fertile window, and a formal semen analysis. Evidence replaces pride.
A woman is not asked if she is relaxed enough. The diagnostic focus centers on cycle regularity, physical ovulation signs, and the alignment of luteinizing hormone tests with cervical mucus changes. The audit investigates severe pelvic pain, dyspareunia, heavy bleeding, or past miscarriage. Finally, the clinical history checks for thyroid symptoms, galactorrhea, prior pelvic infection, historical ectopic pregnancy, and how maternal age changes clinical urgency. Evidence replaces blame.
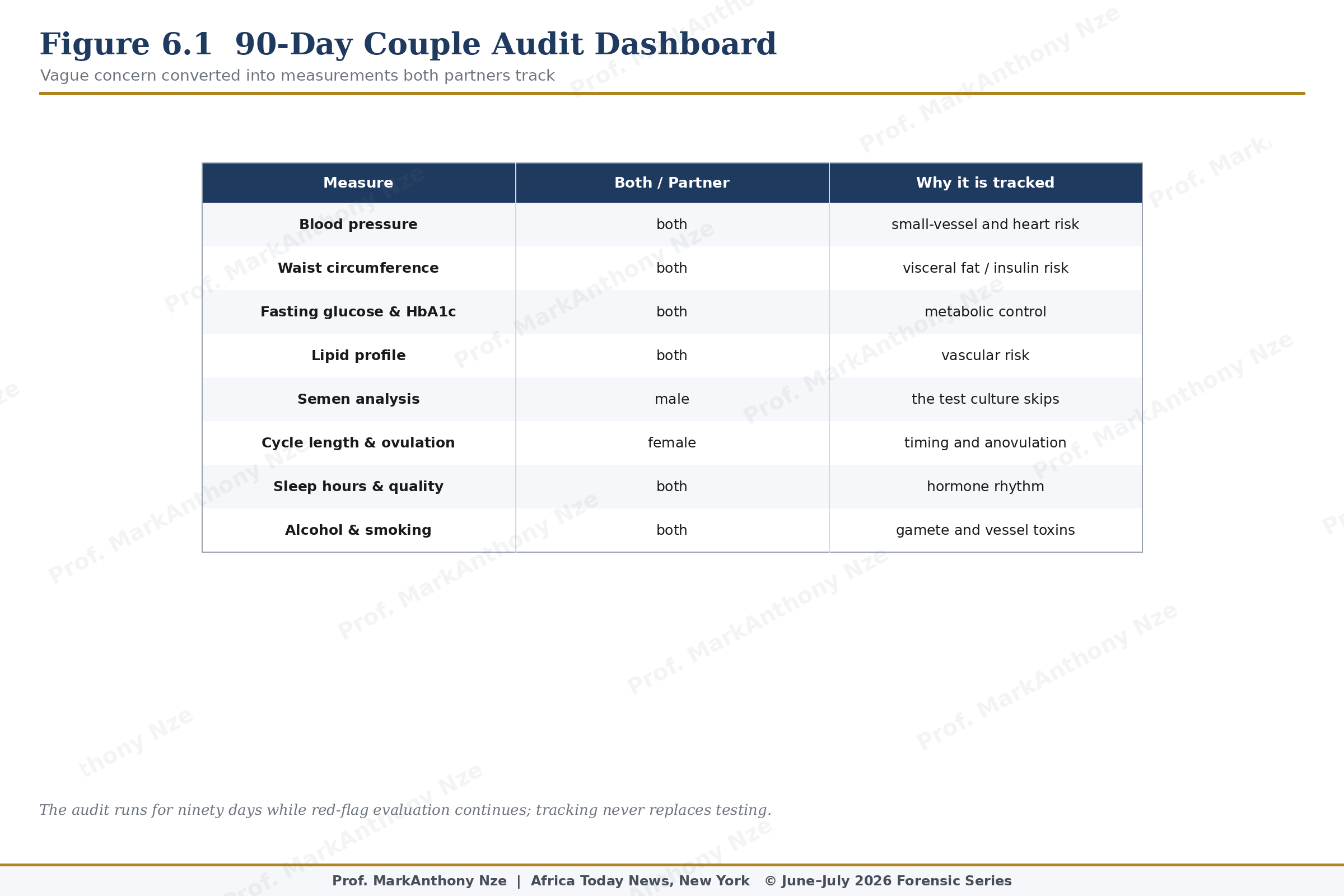
Figure 6.1. 90-Day Couple Audit Dashboard.
Daily entries should be simple enough to survive real life. Sleep duration, sleep quality, exercise, alcohol, smoking or nicotine exposure, intercourse, erectile quality, menstrual bleeding, cervical mucus, LH testing, pelvic pain, medication use, fever, illness, and stress level can be logged without turning the home into a clinic. Weekly entries can include weight, waist, blood pressure, step count or exercise minutes, and symptom notes.
Sex timing belongs in the audit but should not become surveillance. Intercourse every one to two days during the fertile window is often practical, but forced performance can worsen ED and relationship strain. A couple should identify the fertile window using cycle history, cervical mucus, and LH testing where useful, while keeping enough flexibility for fatigue, pain, work, and emotional pressure. Fertility timing should assist sex, not police it.
Semen analysis should not wait until the end of the audit when risk is already visible. A man with prior abnormal semen, testicular history, ED, ejaculation problems, testosterone use, chemotherapy exposure, varicocele, anabolic steroid exposure, diabetes, or infertility over the recommended timeline should be tested early. Ninety days can then become a repair interval around known data rather than a blind ritual.
Read also: The Fertility Repair Series—Part 5
Basic metabolic measurements belong in the same file. Blood pressure, fasting glucose or HbA1c, lipid status, waist circumference, and weight trend can show whether reproductive symptoms are part of cardiometabolic strain. A man with ED and high blood pressure does not need only bedroom advice. A woman with PCOS features and rising waist circumference does not need only cycle-tracking advice. Measurement identifies the enemy.
Food records should avoid moral language. A meal log is not a confession; it is exposure documentation. Protein adequacy, fiber, vegetable intake, ultra-processed food, sugar drinks, late-night eating, caffeine load, and meal timing can alter glucose and weight patterns. A woman with PCOS symptoms and a man with ED may both benefit when insulin stress is seen rather than guessed.
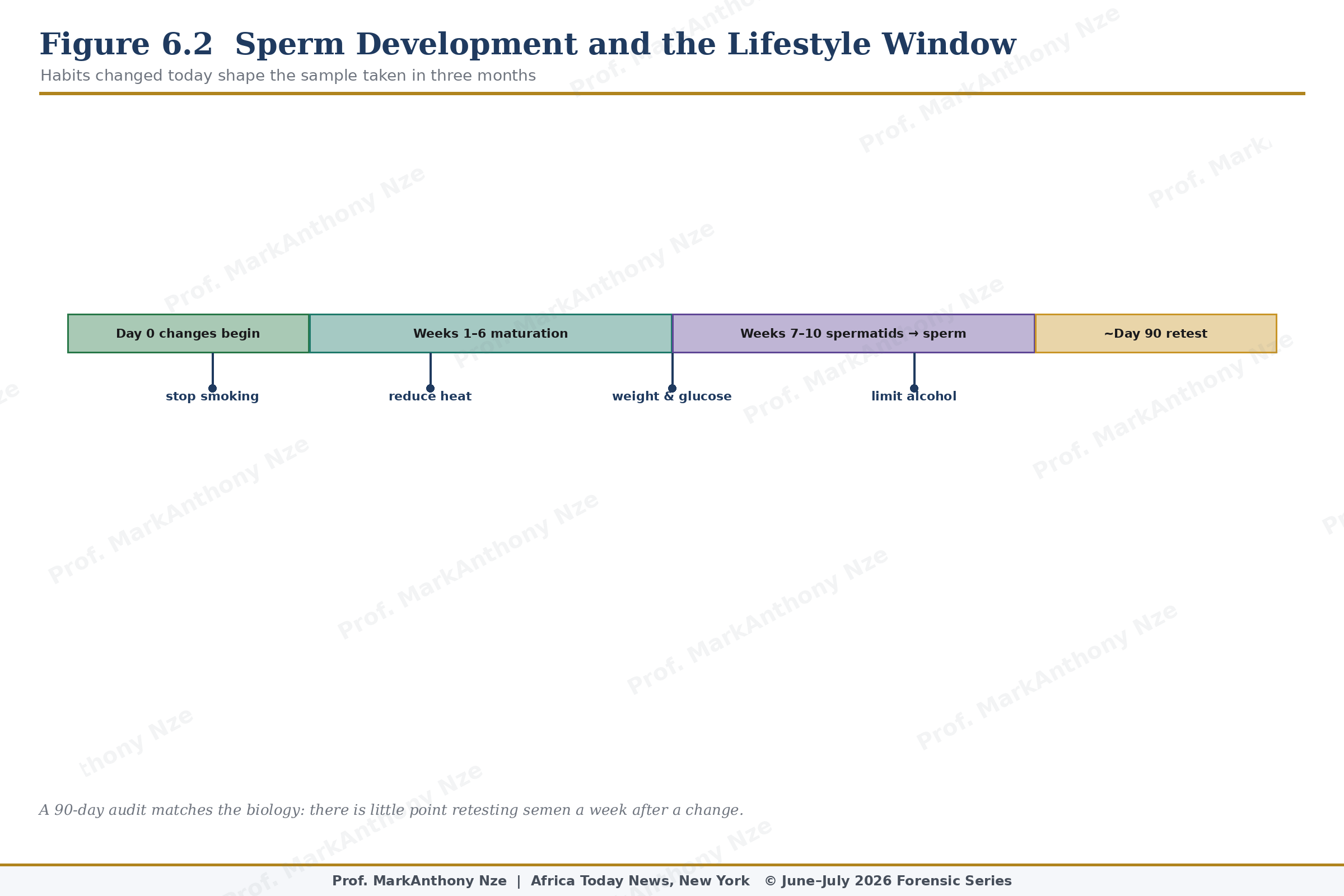
Figure 6.2. Sperm Development And Lifestyle Window.
Sleep audit should be specific. Snoring, witnessed apnea, morning headache, daytime sleepiness, late-night screen exposure, rotating shifts, insomnia, and short sleep can all matter. Poor sleep may worsen insulin resistance, appetite control, mood, testosterone rhythm, libido, and ovulatory stability. A couple that tracks sleep often discovers that reproductive effort is being attempted inside chronic physiological exhaustion.
Alcohol and smoking logs must be honest. Many patients undercount because shame changes memory. Nicotine exposure injures vessels and reproductive cells. Heavy alcohol intake can damage sexual function, sleep, mood, liver metabolism, and hormone balance. Cannabis and recreational substances also belong in the file. Audit work fails when it protects the patient’s preferred self-image instead of recording the body’s exposure.
Pelvic pain must be scored and described. Location, timing, severity, relation to menstruation, bowel symptoms, urinary symptoms, pain with deep penetration, superficial burning, and pain after sex can point toward endometriosis, pelvic-floor dysfunction, infection, ovarian pathology, vulvar disease, or other conditions. A pain diary is not decorative. It can become the document that ends years of dismissal.
Medication review must be written down. Antidepressants, antihypertensives, opioids, sedatives, steroids, finasteride, testosterone, antiandrogens, seizure medicines, chemotherapy agents, and some hormonal drugs can affect sex or fertility. No patient should stop treatment alone, but no fertility audit is complete while medication effects remain unexamined. A prescriber can often distinguish disease burden from drug burden.
Audit conclusions should be written at day 30, day 60, and day 90. Improvements may include more reliable erections, clearer ovulation timing, less alcohol, better sleep, lower blood pressure, reduced waist, improved exercise capacity, less pain, or greater sexual confidence. Alarming findings may include worsening ED, absent ovulation signs, severe pelvic pain, repeated bleeding irregularity, no intercourse possible in the fertile window, or refusal of semen testing.
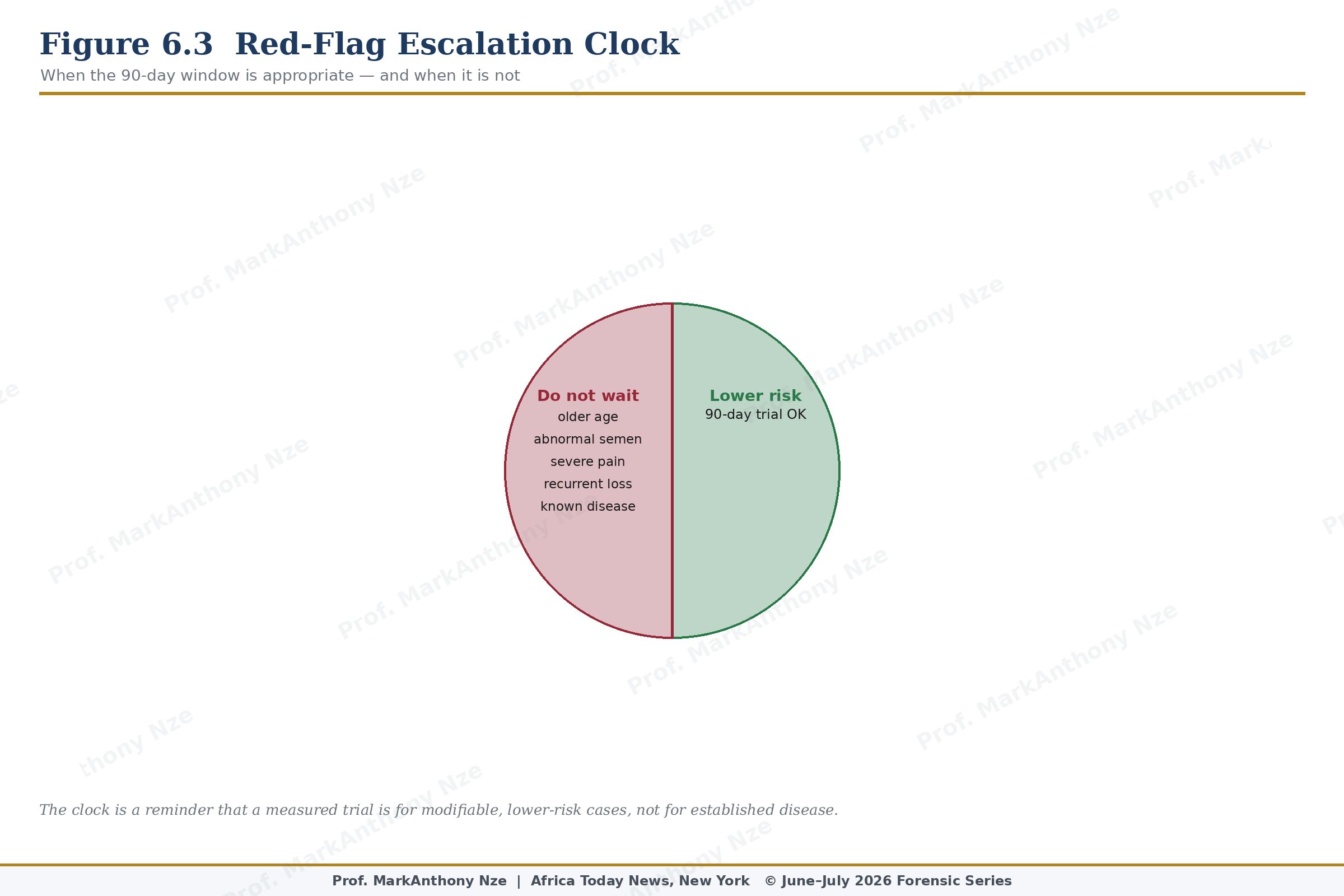
Figure 6.3. Red-Flag Escalation Clock.
Referral rules must be built into the audit from day one. Women 35 or older, women with irregular cycles, known endometriosis, severe pain, prior pelvic infection, suspected tubal disease, recurrent miscarriage, or known ovarian issues may need evaluation before the audit matures. Men with severe ED, cardiovascular symptoms, abnormal semen, testosterone use, testicular abnormalities, or high metabolic risk should not wait for a lifestyle spreadsheet to rescue them.
Read also: The Fertility Repair Series—Part 4
Family pressure should also be logged because it shapes behavior. Couples may avoid clinics to protect privacy, conceal male testing to protect pride, or continue remedies to satisfy relatives. Emotional coercion can become a reproductive exposure. A woman blamed at every family gathering may accept bad advice faster than a woman protected by accurate information. Social injury belongs in the file because it changes medical decisions.
Ninety days ends with classification, not ceremony. Modifiable risks improved, red flags escalated, unknowns measured, sex timing corrected, semen assessed, cycle data organized, and unsafe products removed. Any plan that cannot produce those outputs is not an audit. It is another season of waiting.
A good audit has a cold final page. It lists what improved, what worsened, what remains unknown, what testing is now required, and which remedies are being stopped because they added cost without evidence. That page may be uncomfortable. It is also where reproductive repair becomes adult work.
No couple should leave ninety days with only hope. Hope may survive the process, but data must survive with it: semen, cycle pattern, blood pressure, metabolic status, symptoms, sex timing, pain, sleep, exposure, and referral decisions.
Doctors also benefit from a clean audit. A patient who arrives with three months of cycle dates, ovulation tests, intercourse timing, semen results, blood pressure readings, medication lists, pain scores, sleep notes, and exposure records saves time. Good records do not replace examination, but they sharpen it.
Audit discipline also removes commercial noise. When a couple tracks symptoms and exposures, weak claims become easier to challenge. A capsule that improves nothing after ninety days loses its authority. A sleep change that improves erections earns attention. A cycle pattern that remains irregular despite diet repair points toward evaluation rather than another product.
A couple may discover that the main defect is not biology but access: no nearby lab, no affordable imaging, no specialist, no privacy, no partner cooperation. That discovery is still useful. It turns vague suffering into a named barrier.
Source & Clinical Standards
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.