Stress, Performance Anxiety And The Fertility Clock
Pressure can enter the bedroom as physiology, not mood.
A man who has never once had trouble in bed loses his erection on the single night that matters. His wife has been watching the ovulation strip since breakfast; it turned positive in the late afternoon, and by bedtime the whole evening has quietly become an appointment. Nothing is physically wrong with him. On any ordinary Tuesday his body would have cooperated without being asked. This is not an ordinary Tuesday, and his body seems to know it.
That scene, repeated in thousands of bedrooms, is where stress stops being a mood and becomes physiology. Pressure is not only something a couple feels. The body reads it through the pulse, through sleep that thins out, through a nervous system that stays half-braced for threat. Reproduction does not happen in a laboratory. It happens inside households, marriages, budgets, family histories, religious expectation, and the running commentary of relatives who want to know when the baby is coming.
Performance anxiety in men gets filed under weakness, which is both cruel and wrong. The body’s alarm system works against the calmer signaling that an erection depends on, so a man can have perfectly healthy blood vessels and still fail on command, because the act has turned into an examination. One bad night is enough to plant a fear, and the fear does the rest. By the second or third attempt he is no longer being invited into sex. He is being asked to prove something, and the proving is what defeats him.
Read also: The Fertility Repair Series—Part 10
Women carry a different version of the same weight. The counting begins, and then it does not stop: cycle days, the character of discharge, a basal temperature chart, an app, ovulation strips, every cramp and late period read as possible evidence. Around her, advice arrives that is really surveillance: a mother-in-law’s questions, gossip after church, a colleague’s pregnancy announcement that lands like a verdict. None of this means the problem is imaginary. It means a real clinical event is now lodged inside a nervous system that has not had a quiet week in months.
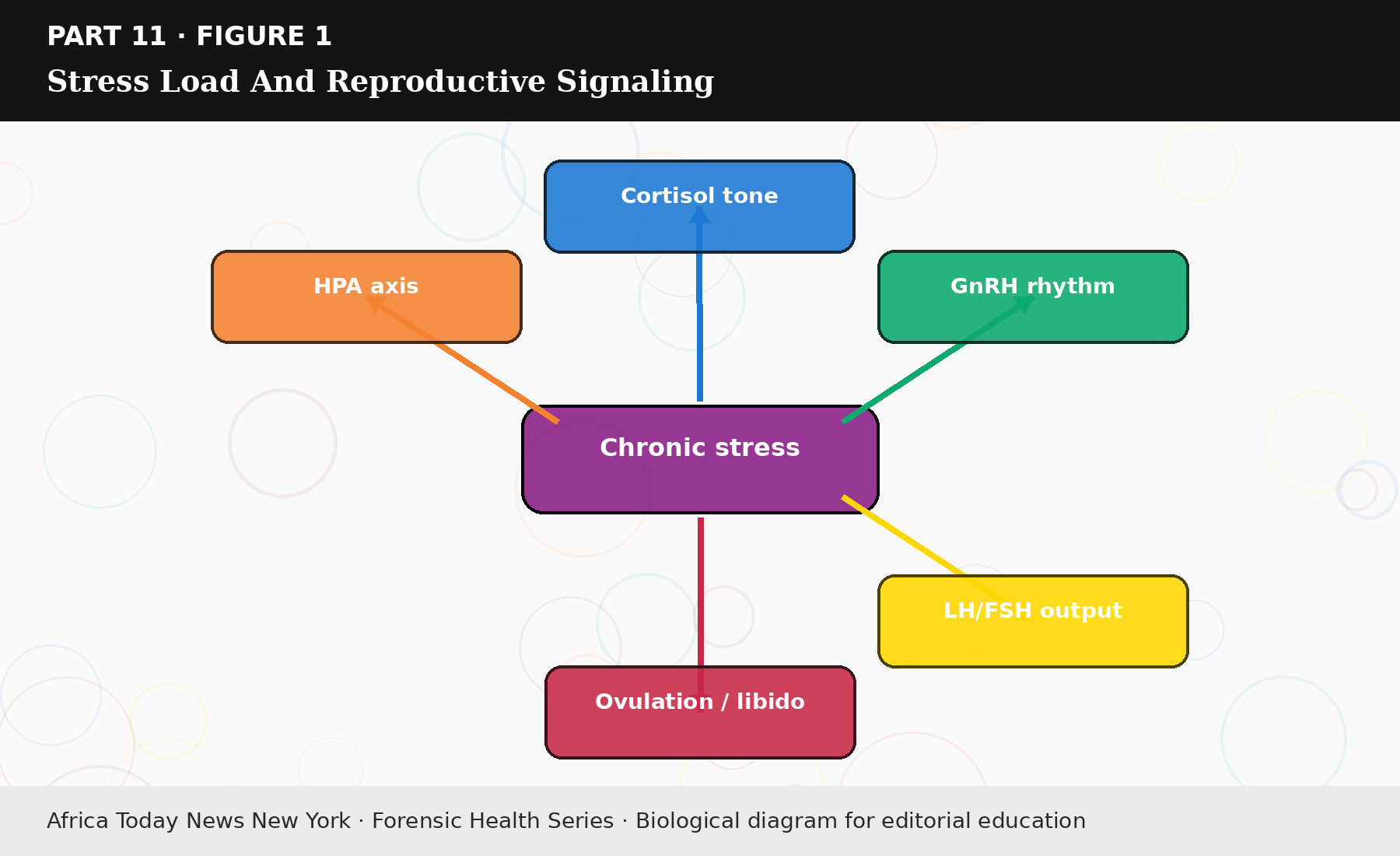
Figure 11.1: Stress Load And Reproductive Signaling.
The medical literature is clear about the direction of cause, and it is worth saying plainly because so many patients have it backward. Infertility and its treatment generate anxiety, low mood, and sexual strain; the distress is mostly a consequence rather than the origin, and psychological support can ease that burden for many patients (Jackson et al., 2025; Simbar et al., 2025). Telling a woman with blocked tubes to relax will not open them. Frightening a man with diabetic erectile dysfunction into silence will not repair his vessels. Blame is not a treatment, and it usually makes the real work harder.
Stress does its quieter damage through the calendar of ordinary life. A couple under pressure eats at odd hours, drinks a little more, sleeps a little less, argues, lets the exercise habit lapse, and sometimes misses the appointments that would actually move things forward. Occasionally they reach for an unregulated product that promises a faster result than the clinic can. No single cortisol reading captures any of this. A disrupted routine does, which is why careful fertility work treats mental strain as operational evidence rather than background noise.
Read also: The Fertility Repair Series—Part 9
There is a real discipline in mapping a failed encounter the way one would map any recurring incident. What happened in the hour beforehand? Was the attempt tied to a positive ovulation test, and had there been alcohol, a short night, an argument? Did a previous failure leave a residue of dread? The questions are not romantic, but a year of unexamined disappointment is worse, and this kind of inventory tends to point at something fixable.
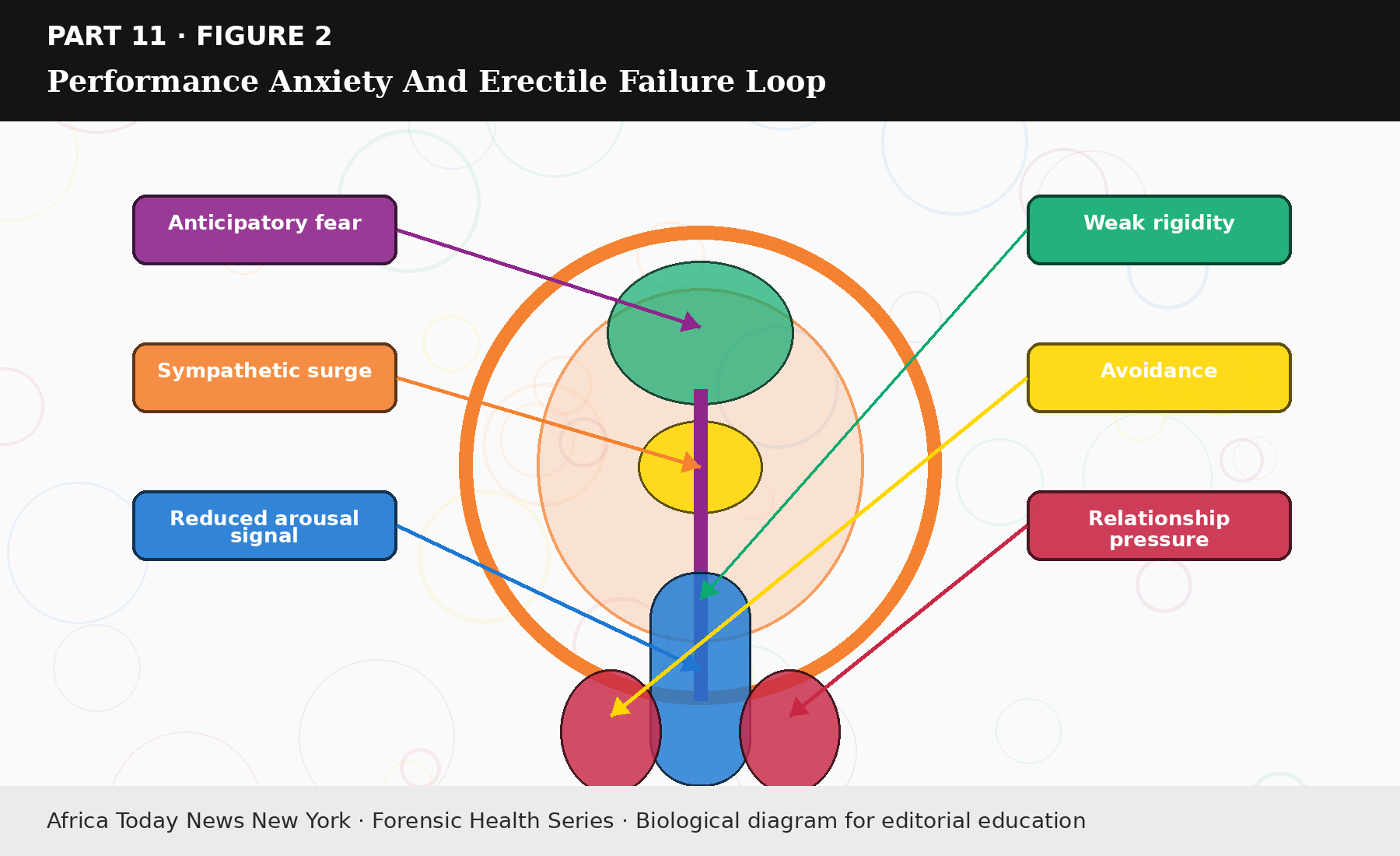
Figure 11.2: Performance Anxiety And Erectile Failure Loop.
Repair begins by taking unnecessary threat out of the routine. A couple needs a shared plan that keeps sex from collapsing into reproductive labor. Fertile-window timing can stay; what has to survive alongside it is ordinary tenderness, touch that carries no demand, intimacy on days when nobody is counting. Men whose erections have become unreliable deserve a cardiovascular and metabolic check when the history warrants it, and they also deserve a space where one soft night is not treated as a referendum on their manhood. Women with pelvic pain need evaluation, not an instruction to endure intercourse for the sake of the schedule.
Breathing practice, counseling, steadier sleep, moderate exercise, prayer, and honest conversation between partners can each help, depending on the couple. None of them should be sold as a cure. Their job is narrower and more honest: to lower the body’s alarm, protect sex, interrupt avoidance, and keep medical decisions from being made in a panic. Psychological care does not replace a semen analysis, a tubal assessment, thyroid testing, or an endometriosis work-up. It is what keeps a couple standing while those facts are gathered.
Money belongs in this conversation, because financial strain turns biological. Evaluation, imaging, and repeated visits are expensive, and the delay they cause has consequences of its own. A woman buys herbs because an ultrasound costs more than she has that month. A man buys a stimulant because a urology visit feels both humiliating and unaffordable. Poverty does not make the fraud less harmful, but it explains why so many walk into it, and any advice that ignores the price of care is not really advice.
Ninety days of stress repair should be judged by what a couple does, not by how inspired they feel. Sleep, alcohol, cigarettes, walking, how often sex happens and how reliably it works, pain, the arguments that erupt around fertile days: these are the things worth writing down. If the tracking itself is feeding the anxiety, simplify it. If intercourse collapses every fertile window, then erectile function, pain, and performance fear need to leave the bedroom and enter a clinical conversation. If relatives are poisoning the marriage, then managing what they are told becomes part of the treatment.
A small household rule lowers the temperature faster than most interventions: no fertility argument starts in bed. Testing, money, appointments, ovulation kits, and disappointed relatives get discussed somewhere else, with clothes on. A bedroom stops being safe when every touch is followed by negotiation, and arousal needs a little safety before it returns.
Clinics can deepen the strain without intending to, by treating the couple as two separate patients. She gets cycle monitoring and pelvic imaging while his semen test keeps being postponed; he leaves with a prescription for erectile dysfunction while nobody asks whether fertile-window sex has become a public trial. Each half-finished file breeds more uncertainty, and uncertainty breeds the rituals and the exhaustion that follow. What most couples need is one shared reproductive record rather than two private folders of shame, and building that record early does more for the nervous system than any calming technique.
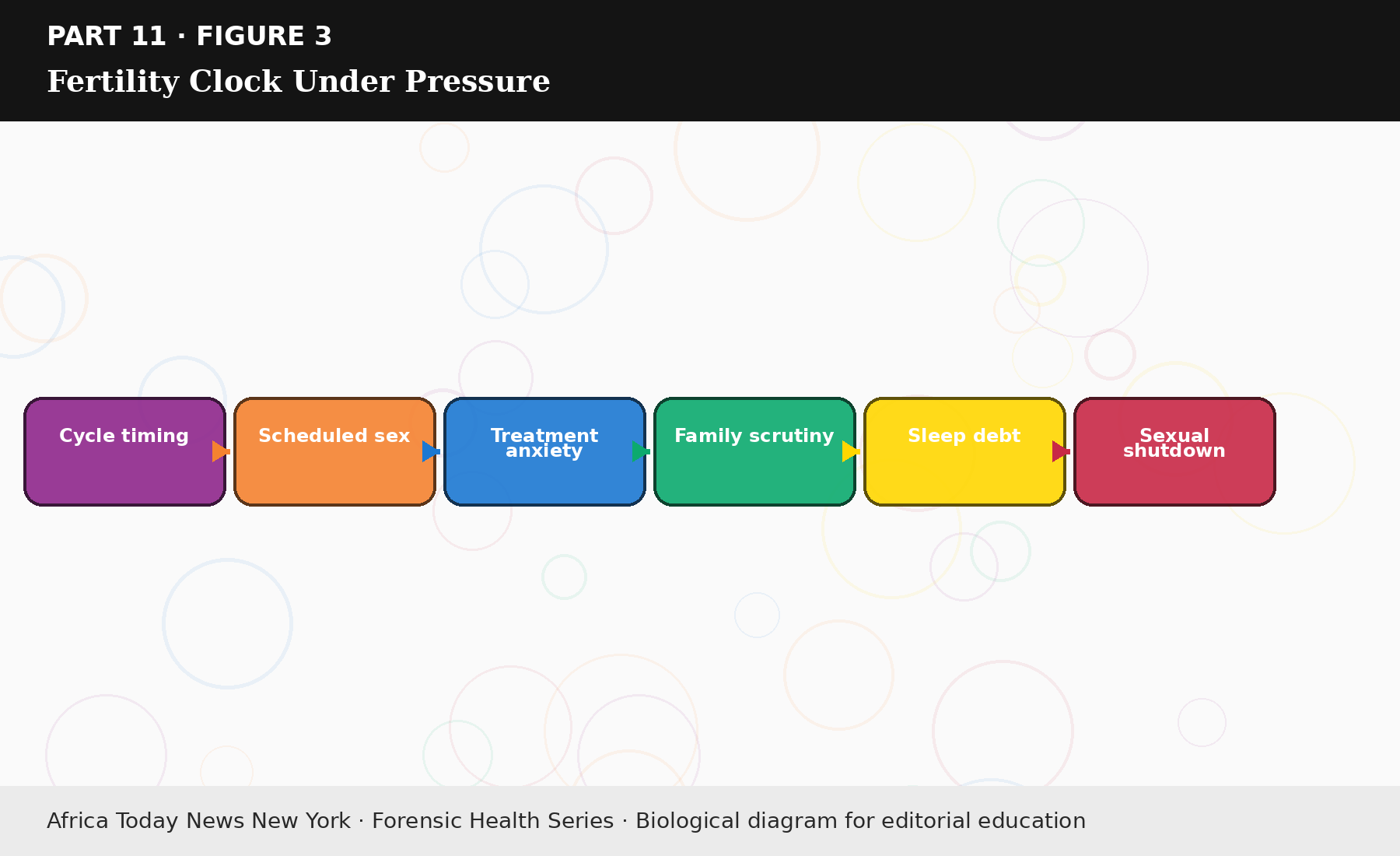
Figure 11.3: Fertility Clock Under Pressure.
Pressure is not the cause of every infertility case. Plenty of couples conceive under enormous strain, and plenty of calm couples do not. What pressure reliably does is decide how a case is handled: whether a man agrees to be tested, whether a woman feels safe enough to say that sex hurts, whether the two of them keep working together or retreat into separate, frightened corners. That is the part worth managing, and most of it is within reach.
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.