
When Natural Remedies Are Not Enough
Delay is no holistic. It is clinical loss with nicer language.
Natural care becomes harmful when it is used to postpone diagnosis. A couple may improve diet, sleep, exercise, sex timing, toxin exposure, and stress while still needing semen analysis, pelvic imaging, endocrine testing, cardiovascular assessment, tubal evaluation, or reproductive endocrinology care. Those paths are not enemies. Delay begins when lifestyle work is sold as a substitute for evidence.
Erectile dysfunction carries the first public warning. Sudden or progressive ED in a man with diabetes, hypertension, smoking history, obesity, dyslipidemia, chest symptoms, shortness of breath, poor exercise tolerance, or nitrate medication use deserves medical assessment. Princeton IV consensus work places ED inside cardiovascular risk evaluation because it can signal vascular disease (Kloner et al., 2024). A supplement plan that ignores this possibility is risk concealment.
Severe or new ED should also raise questions about medication effects, neurologic disease, pelvic surgery, prostate treatment, low testosterone, depression, sleep apnea, alcohol burden, and unregulated sexual products. FDA warnings on contaminated sexual-enhancement products make one point unavoidable: natural labeling cannot be trusted as proof of safety. Hidden drug ingredients can place vulnerable men at serious risk, especially those with cardiovascular disease or nitrate prescriptions.
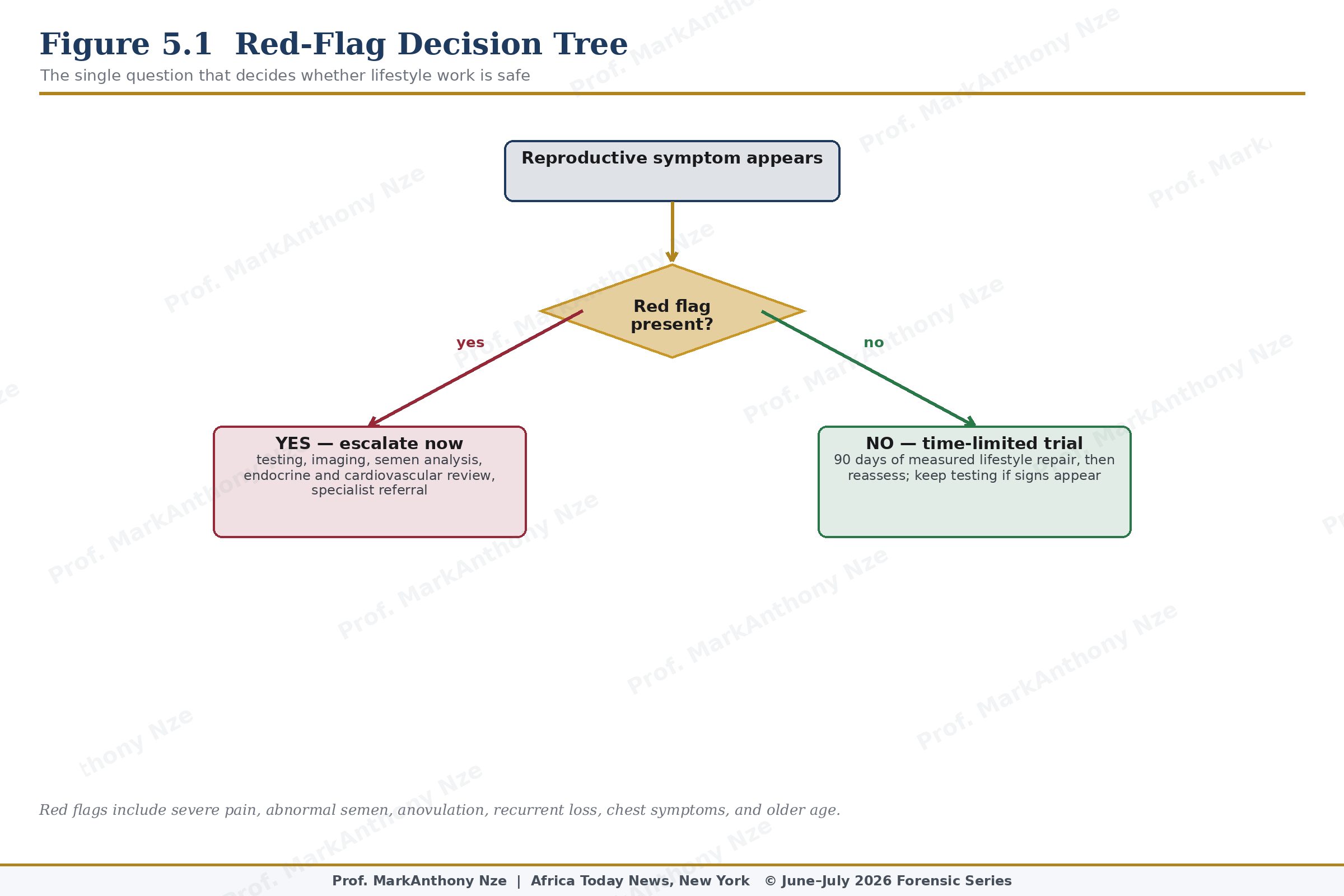
Figure 5.1. Red-Flag Decision Tree.
Female infertility has its own escalation rules. ASRM guidance supports evaluation after 12 months of regular unprotected intercourse for women under 35, after 6 months for women 35 or older, and earlier when symptoms or history suggest reproductive disease. Earlier evaluation is not impatience. It is time protection. Irregular cycles, amenorrhea, known or suspected PCOS, severe menstrual pain, deep pain with sex, prior pelvic inflammatory disease, suspected tubal disease, recurrent miscarriage, chemotherapy exposure, ovarian surgery, or known male-factor risk should shorten the waiting period.
Cardiovascular urgency deserves special handling because sexual embarrassment can hide danger. ED with chest pain, exertional symptoms, fainting, severe shortness of breath, uncontrolled blood pressure, or nitrate medication use is not a supplement question. It is a medical-risk question. Men should not be sent toward hidden-drug products while their arterial status remains unknown.
Blocked tubes do not respond to teas. Hydrosalpinx, tubal occlusion, significant pelvic adhesions, and severe endometriosis are anatomical or inflammatory problems requiring diagnosis. A woman with prior ectopic pregnancy, pelvic infection, untreated chlamydia or gonorrhea history, pelvic surgery, ruptured appendix, or endometriosis symptoms may need imaging or specialist evaluation. Guessing at ovulation timing while the route is blocked wastes months.
Uterine cavity distortion also resists wellness language. Submucosal fibroids, significant cavity-distorting fibroids, polyps, adhesions, and some congenital uterine anomalies may affect implantation or miscarriage risk. Nutritional repair may improve anemia or metabolic status, but it does not redraw the cavity. Ultrasound, saline sonography, hysteroscopy, MRI in selected cases, or specialist review may be needed depending on symptoms and suspected anatomy.
Endometriosis demands particular caution because patients are often conditioned to endure pain. Severe dysmenorrhea, deep dyspareunia, chronic pelvic pain, bowel pain with menstruation, urinary pain with cycles, infertility, or persistent pelvic symptoms deserve evaluation. Pain that repeatedly disables a woman is not temperament. It is evidence. When disease is suspected, a longer supplement trial can become a form of neglect.
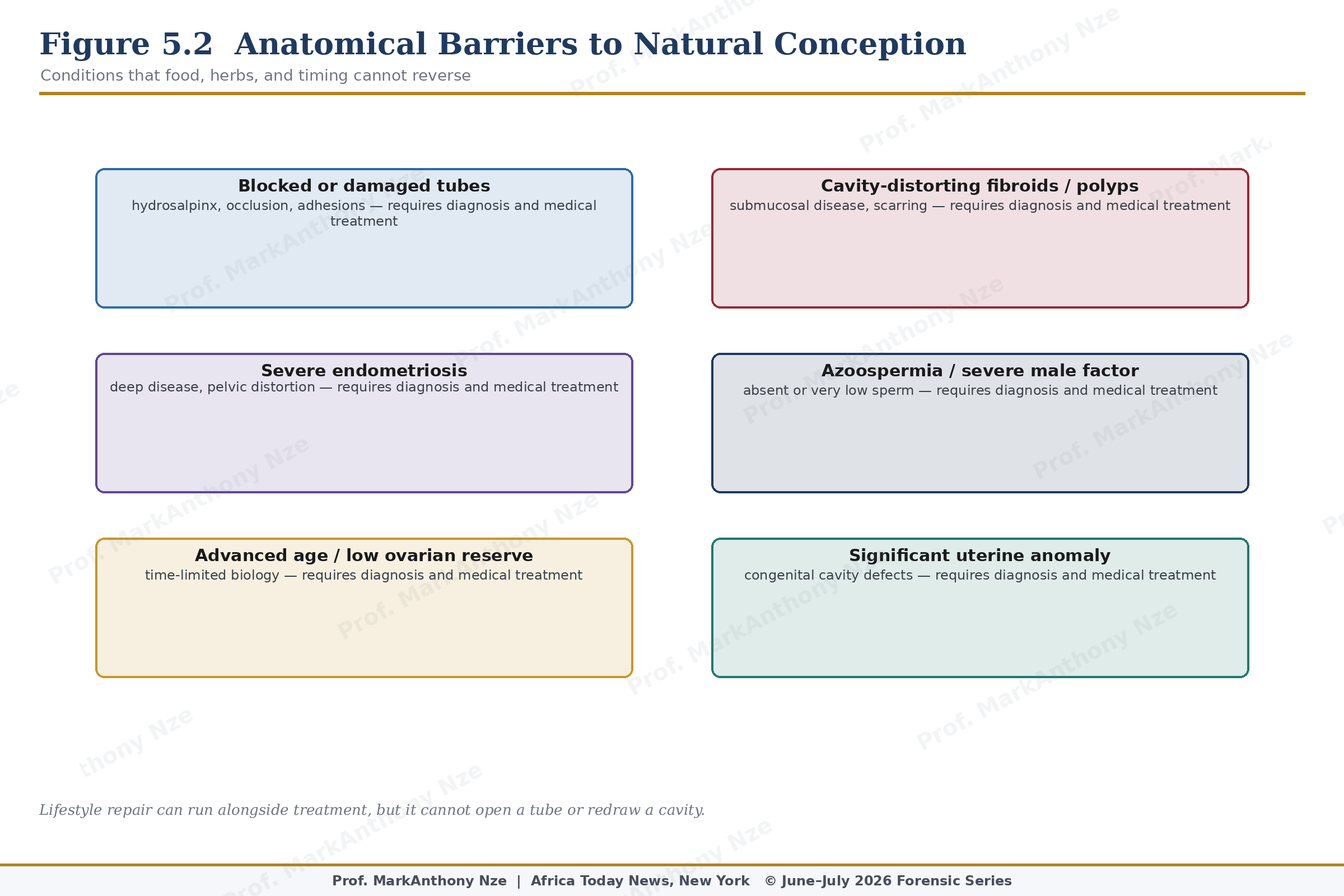
Figure 5.2. Anatomical Barriers To Natural Conception.
Age does not make pregnancy impossible, but it changes the price of delay. A woman over 35 does not need panic, yet she deserves faster evaluation than a much younger woman with no warning signs. A woman over 40 who is told to spend another year on teas has received advice that ignores ovarian biology. Kindness without timing is not kindness.
Read also: The Fertility Repair Series—Part 3
Endocrine red flags are equally direct. Irregular or absent periods, galactorrhea, unexplained headaches, visual symptoms, marked acne or hirsutism, sudden weight changes, cold or heat intolerance, recurrent miscarriage, or suspected ovulatory failure can point toward thyroid disease, prolactin excess, PCOS, hypothalamic dysfunction, premature ovarian insufficiency, adrenal disorders, or other hormonal disease. Herbal hormone balancing should not precede basic evaluation when symptoms are visible.
Male-factor red flags include abnormal semen analysis, very low sperm concentration, absent sperm, low volume, testicular asymmetry, small testes, varicocele, prior undescended testes, chemotherapy or radiation exposure, anabolic steroid use, testosterone therapy, sexual dysfunction, retrograde ejaculation, genital infection history, and occupational exposures. Specialist referral may be needed because some male causes are treatable while others require assisted reproduction or genetic counseling.
Repeated pregnancy loss deserves investigation rather than superstition. Age-related chromosomal risk, uterine cavity problems, thyroid disease, diabetes, antiphospholipid syndrome, genetic factors, and other medical causes may need assessment. Telling a couple to try again after repeated losses without review may preserve tradition, but it does not respect evidence. Grief should not be managed with vagueness.
Pain is one of the most mismanaged red flags. Severe period pain, deep pain with intercourse, pelvic pain outside menstruation, bowel pain during cycles, or chronic urinary-pelvic symptoms may point toward conditions that require medical workup. A patient who repeatedly misses work, avoids sex, or lives around menstrual suffering should not be told that pain proves womanhood.
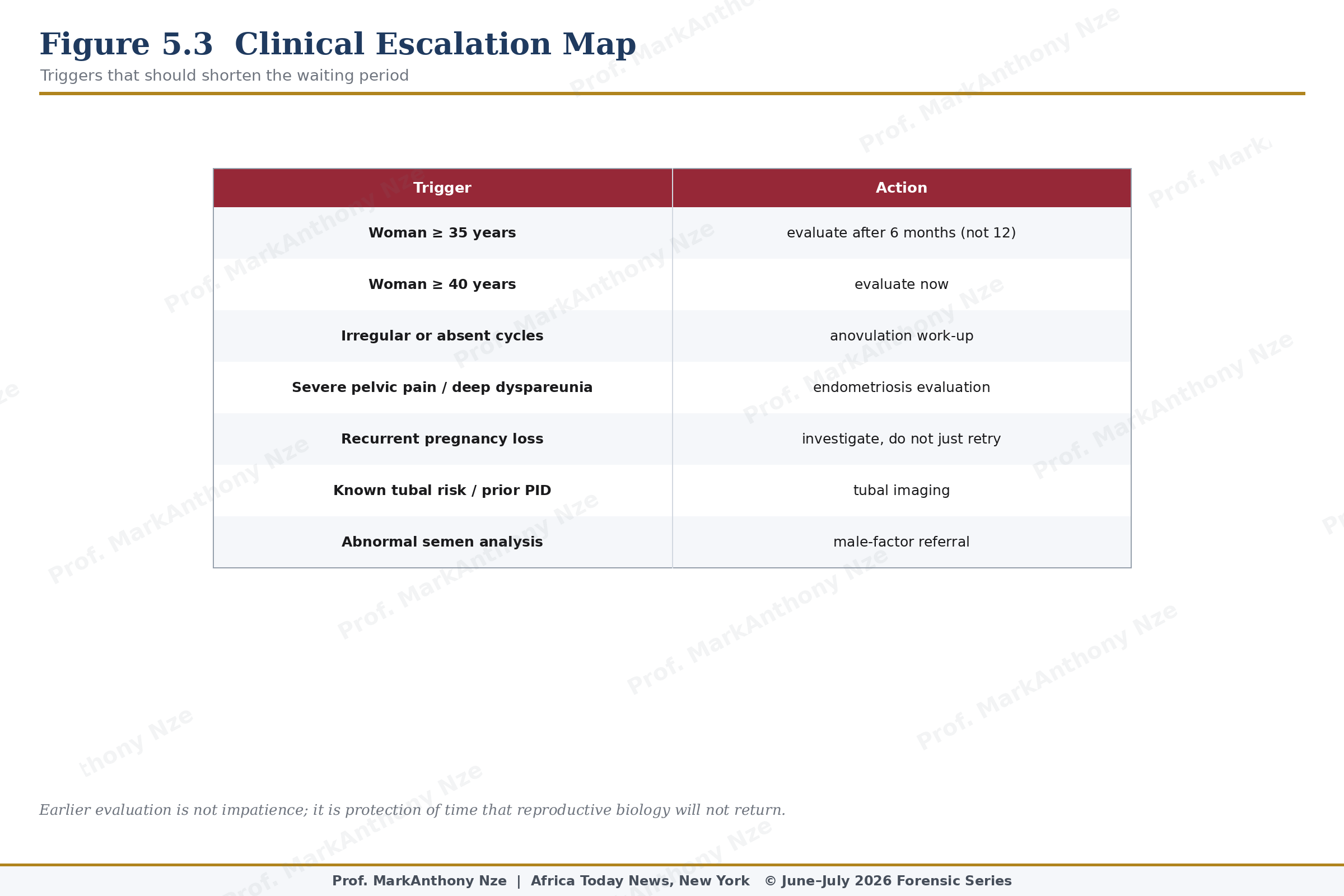
Figure 5.3. Clinical Escalation Map.
Natural care still belongs in the plan after red flags appear. A man can begin walking, reduce alcohol, stop smoking, improve sleep, and address weight while cardiometabolic testing proceeds. A woman can start folic acid (U.S. Preventive Services Task Force, 2023), regulate food quality, reduce toxins, track cycles, and improve metabolic health while pelvic imaging is scheduled. A couple can improve sex timing while semen testing is ordered. Lifestyle work supports the patient; it should not barricade the clinic door.
Financial barriers must be named. Many readers delay care because consultation, imaging, semen analysis, fertility treatment, and medication are expensive or geographically inaccessible. That reality does not make unverified remedies effective. It means public health has failed many couples. Responsible writing should provide low-cost first steps without pretending that poverty changes anatomy.
Cultural pressure also fuels dangerous waiting. Families may blame the woman, men may resist semen testing, religious communities may frame infertility as punishment, and friends may recommend herbs with absolute certainty and no evidence. Online sellers may use African, Asian, or indigenous language to cloak commercial extraction. Respect for tradition does not require obedience to false claims.
Read also: The Fertility Repair Series—Part 4
A serious rule governs this series: natural repair is strongest when it is measured, time-limited, and paired with diagnosis. A 90-day audit may be reasonable for modifiable risks in lower-risk cases. It is not reasonable when age, severe symptoms, known disease, repeated loss, or major male-factor suspicion already demands escalation. Time is reproductive tissue.
Medical care is not an admission that nature failed. It is an admission that biology has specific mechanisms, and some mechanisms require tools beyond food, sleep, exercise, and plants. Honesty protects the patient from both medical arrogance and wellness fraud.
Escalation is not defeat. Escalation means the audit has located a boundary. At that boundary, the correct act is not more powder, more secrecy, or more months. It is measurement, imaging, referral, treatment discussion, and informed choice.
A publication carrying this series must be legally and clinically clean on that point. Natural intervention can support physiology, but it cannot replace diagnosis when red flags are present. Readers deserve that line because sellers will not draw it for them.
Warnings must be printed in language readers can use. Seek care early for severe pain, irregular or absent cycles, repeated miscarriage, infertility past age-based thresholds, known tubal risk, sudden ED, chest symptoms, abnormal semen, testosterone use, or contaminated supplement exposure. Delay becomes dangerous when the body has already shown a red flag.
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.