Pelvic Floor Secrets Men Are Rarely Taught
A pelvis can be weak, guarded, painful, or neurologically overprotective.
Male pelvic-floor dysfunction hides behind vocabulary before it ever hides behind anatomy. Men grow up learning about biceps and stamina and testosterone, and almost none of them are told about the sling of muscle, fascia, and nerve beneath the pelvis that helps run urination, bowel movements, ejaculation, erection support, and simple pelvic stability. When that region stops behaving, the trouble can surface almost anywhere nearby: the penis, the testicles, the bladder, the rectum, the lower belly, the hips, the back. A man goes looking for a prostate problem or a testosterone problem and never suspects the floor of his own pelvis.
Kegels became the reflex answer because weakness is easy to name and easy to sell. Some men do benefit from strengthening, especially after prostate surgery or with clear urinary leakage. Plenty of others have the opposite problem, a pelvic floor that is overactive, guarded, and unable to let go. Telling every man with erectile trouble or premature ejaculation to squeeze harder can make things worse when tension is already the disease. The muscle does not need more tone; it needs to learn how to release.
Overactive, hypertonic patterns tend to keep company with anxiety, chronic stress, heavy lifting, long hours of sitting, cycling pressure, constipation, and a history of pelvic or sexual fear. A man will describe “erection trouble” while the deeper story is a pelvis that never comes off high alert. Blood flow, nerve signaling, and attention all get pulled into the same clench, and sex becomes one more place where the nervous system refuses to stand down.
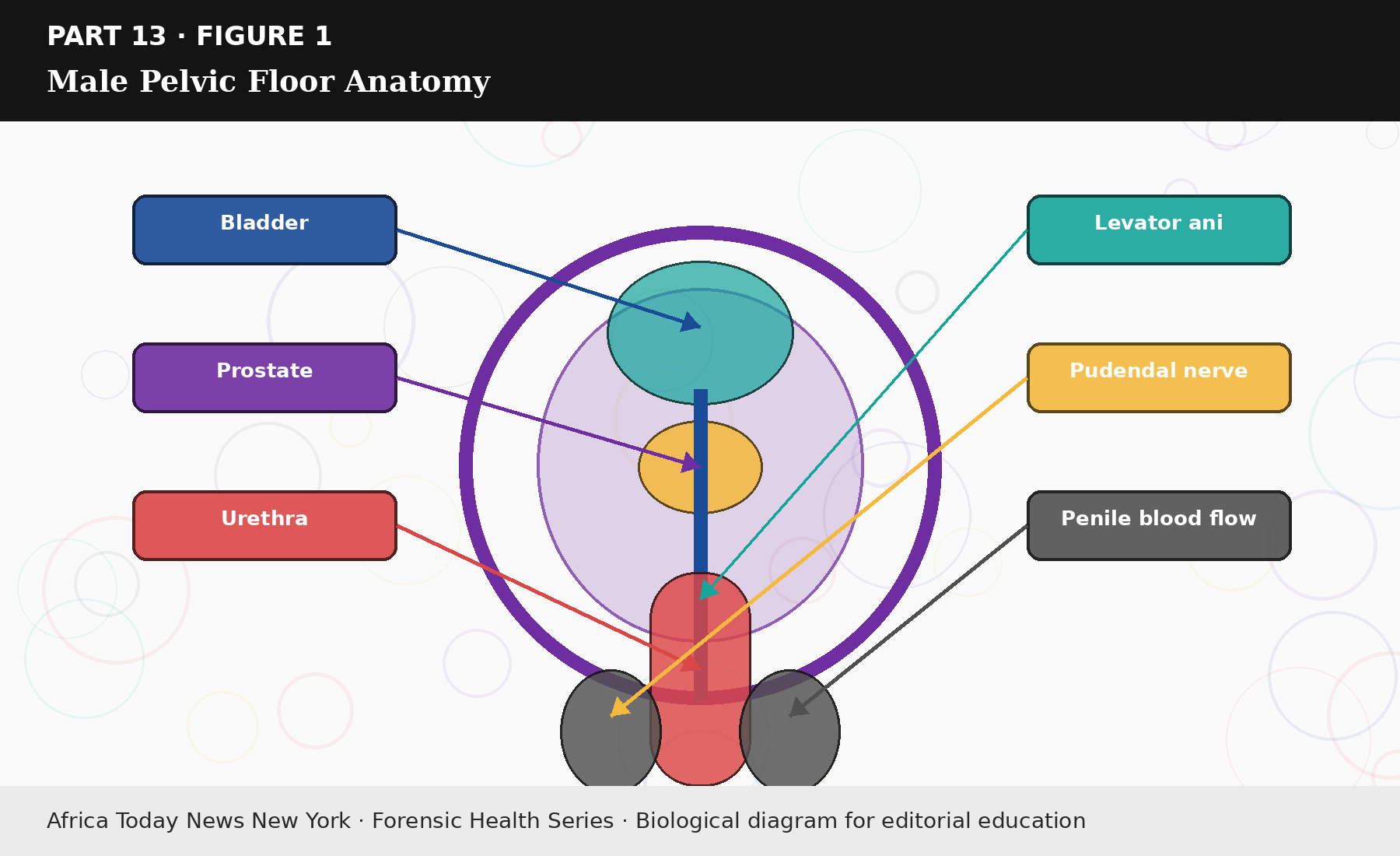
Figure 13.1: Male Pelvic Floor Anatomy.
Assessment matters here because self-diagnosis is close to useless. A pelvic-floor physical therapist or a clinician trained in pelvic pain can evaluate muscle tone, tenderness, coordination, breathing, posture, hip mobility, and the bowel and urinary picture, then sort out what is actually driving the symptoms. Reviews describe pelvic physical therapy as a promising avenue for male sexual disorders, with the caveat that results depend heavily on the underlying cause and on individualized care (Sahin et al., 2025). One man needs strengthening. Another needs the reverse: relaxation, manual therapy, breathing work, and some nervous-system retraining before any strengthening would be safe.
Erectile dysfunction tied to the pelvic floor rarely shows up by itself. A man may also report a bladder that never feels empty, urinary urgency or hesitancy, constipation, aching in the perineum, numbness, pain after ejaculation, tight hips, or a discomfort that seems to wander. None of that rules out vascular disease, diabetes, low testosterone, medication effects, or depression. It simply adds another file to the stack, and a careful plan keeps every plausible cause visible until the evidence clears them off one by one.