Case File: Male Endocrine
Male Hormones Without Dangerous Shortcuts
Testosterone can restore a man’s confidence in bed and quietly switch off the very cells that make him a father.
Low testosterone is sold to a man as a verdict on his manhood long before it is confirmed as a finding in his blood. He arrives with a familiar bundle — flat libido, fewer morning erections, fatigue, a thickening waist, broken sleep, a low mood he cannot name — and the marketplace is ready before the diagnosis is. Injections, gels, “boosters,” imported capsules, and the whispered protocol of a back-street men’s clinic all arrive within the week. Sperm is mentioned late, if it is mentioned at all. That sequence is exactly backwards, and reversing it is the whole discipline of this chapter.
Begin with a distinction that most advertising is designed to blur: the testosterone in a man’s bloodstream is not the testosterone inside his testis. Sperm production depends on a continuous conversation running from brain to groin. The hypothalamus releases GnRH in pulses; the pituitary answers with two messengers, LH and FSH; LH drives the Leydig cells to manufacture testosterone inside the testis at concentrations many times higher than the blood ever sees; FSH instructs the Sertoli cells to nurse immature germ cells through the long assembly line of spermatogenesis. Intratesticular testosterone is the non-negotiable fuel of that line. Take testosterone from the outside and the blood level rises, but the brain reads that surplus as a signal to stop asking — LH and FSH fall, the Leydig cells go quiet, intratesticular testosterone collapses, and the assembly line stalls. A man can feel sharper while his semen report is being emptied out beneath him.
Read also: The Fertility Repair Series III—Overview
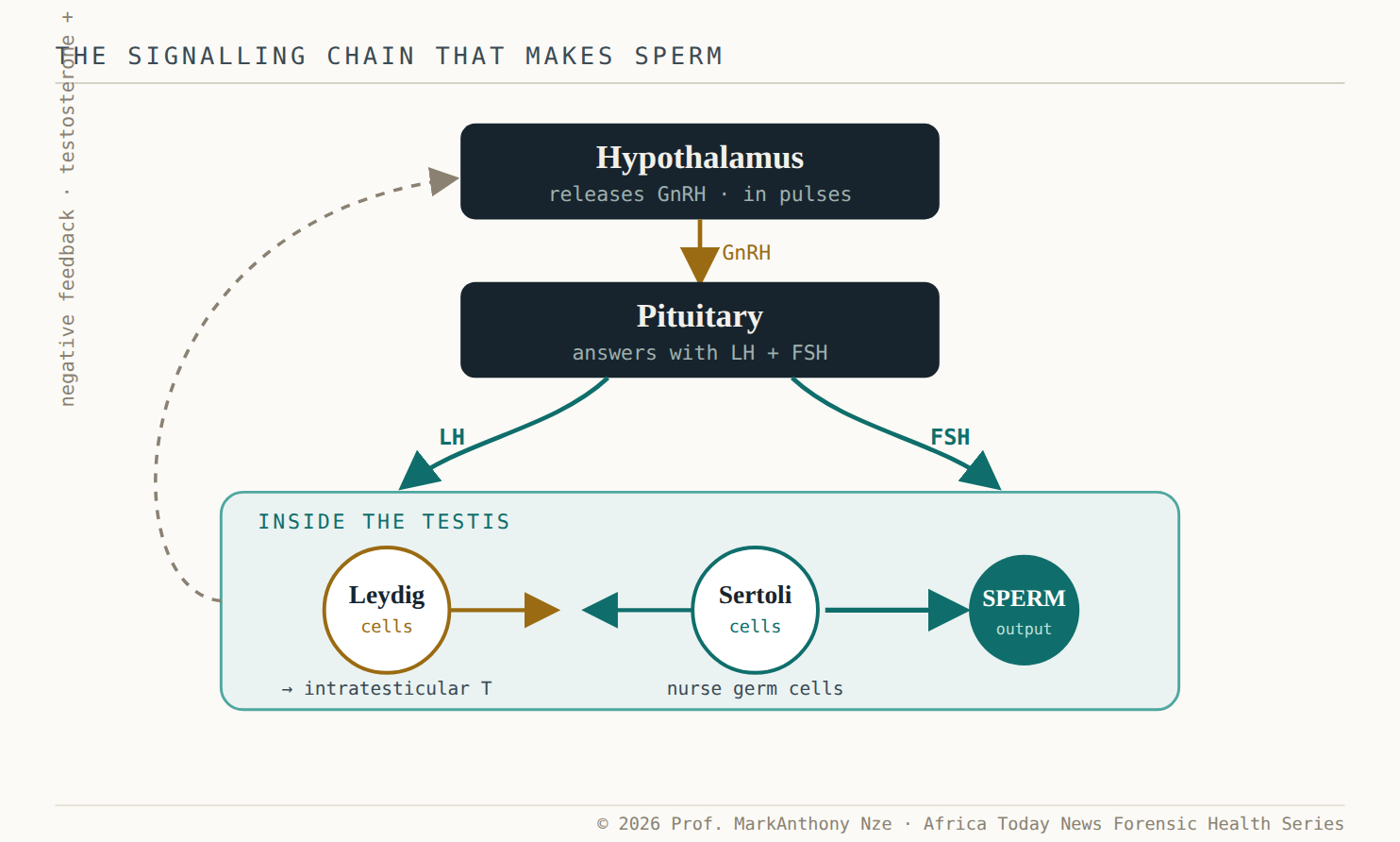
Fig. 21.1 The signalling chain that makes sperm. Brain and testis stay in constant conversation. The fuel for sperm is testosterone made inside the testis — not the level measured in a blood tube.
The shortcut that backfires
This is why the 2024 AUA/ASRM guideline is not squeamish. Its instruction to clinicians is a Clinical Principle — its firmest tier of advice — and it reads plainly: for any man interested in current or future fertility, do not prescribe exogenous testosterone. The same guidance folds anabolic steroids, prohormones, and hidden hormone exposure into the core evaluation, because they act by the identical mechanism as a prescription: they suppress the pituitary and starve the testis of its own signal. The dose does not have to be exotic. Even supraphysiological injections do not reliably guarantee azoospermia in every man, but they drive sperm counts down in effectively all of them — which is precisely the wrong bet to place on a wanted pregnancy.
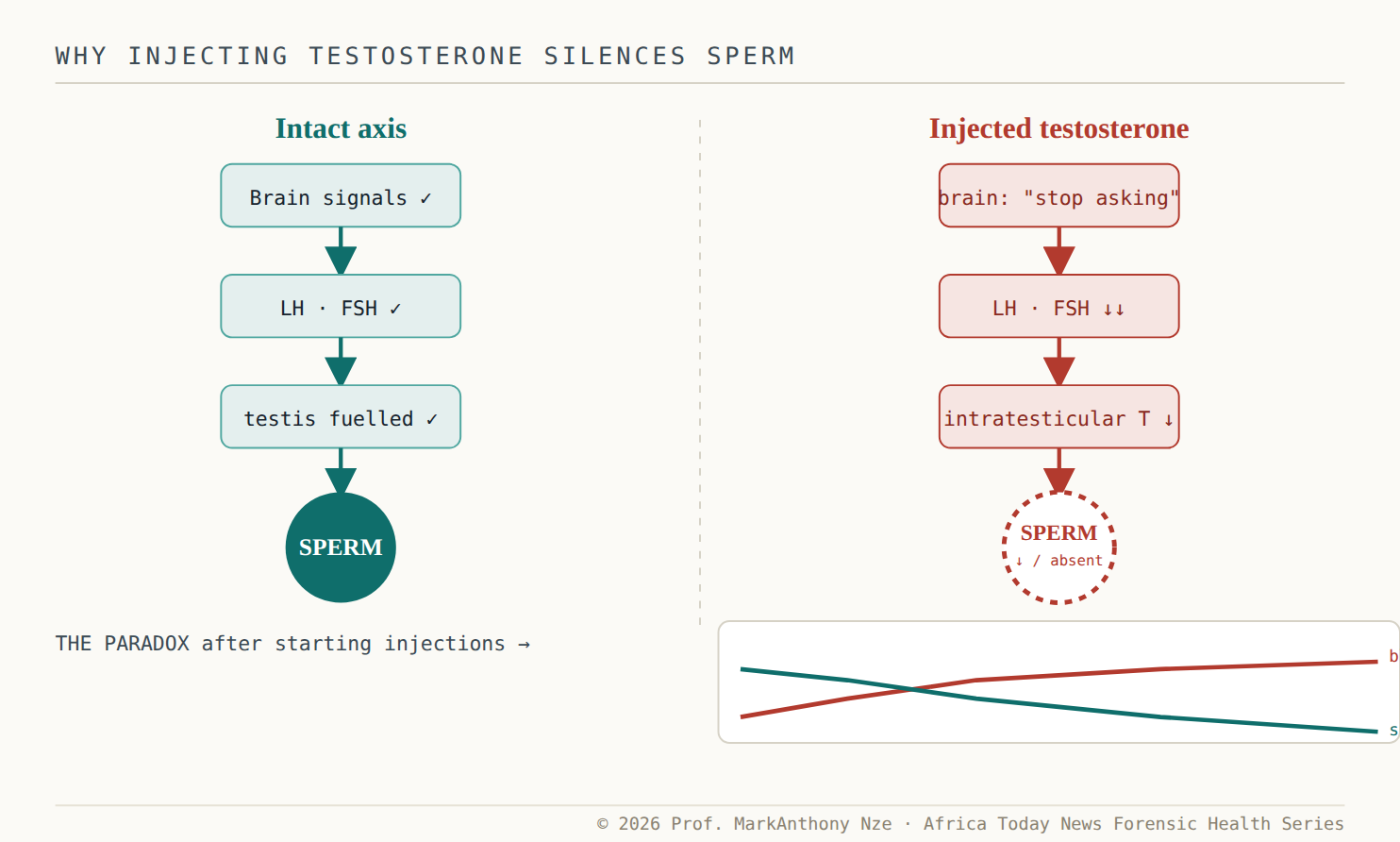
Fig. 21.2 The paradox in one picture. The blood number climbs while the sperm line falls. A man reading only his testosterone level sees success; the semen report tells the opposite story.
None of this means a struggling man should be dismissed. Genuine hypogonadism is real, and telling a symptomatic patient that fertility is “theoretically possible” is not care. The point is that the symptoms deserve a diagnosis before they deserve a drug. Much of what presents as low testosterone is downstream of something else entirely: visceral fat and insulin resistance, untreated obstructive sleep apnoea, heavy alcohol, opioids and other medications, depression, chronic illness. The man snoring through unrefreshing nights, waking with a headache and a soft libido, may not need a hormone at all — he may need his airway treated, his weight addressed, his prescriptions audited. A shortcut here does not correct the upstream injury; it hides it.
Read also: The Fertility Repair Series—Part 20
The “natural” boosters exploit the same hunger with weaker evidence and looser quality control. A capsule may hold a mineral that helps only the man who was deficient in it, a herb of uncertain dose, a stimulant that imitates energy for an afternoon, or — the recurring scandal of this market — an undeclared drug-like compound the label never names. A product that lifts confidence is not proof that anything hormonal was corrected, and a bottle promising masculinity “without side effects” is making a marketing claim, not a physiological one. The tragedy is ordinary: months are spent, money is gone, and the semen was never tested. Meanwhile the genuinely useful moves — resistance training, adequate protein, weight loss where it is needed, repaired sleep, treated metabolic disease — are unglamorous, slow, and real. They shift energy balance, muscle mass, insulin signalling, and inflammatory load without deliberately jamming the pituitary signals that fertility runs on.
Measure first, name the cause
So the method inverts the marketplace. Before any treatment, a man who wants children should have a baseline semen analysis, because it sets a reference point before hormones, illness, or surgery rewrite the file — and an abnormal report changes the entire conversation at once. The hormone work is disciplined too: total testosterone drawn in the morning and repeated when low, never sentencing a man on a single afternoon value taken after a bad night. LH and FSH are interpreted together to locate the problem in the brain or the testis; prolactin and pituitary review follow when the picture demands it; the testes are actually examined. Guidelines specifically direct clinicians to obtain FSH and testosterone for infertile men with low libido, erectile dysfunction, low sperm counts, or small testes. Diagnosis moves more slowly than advertising, and that is the feature, not the flaw.
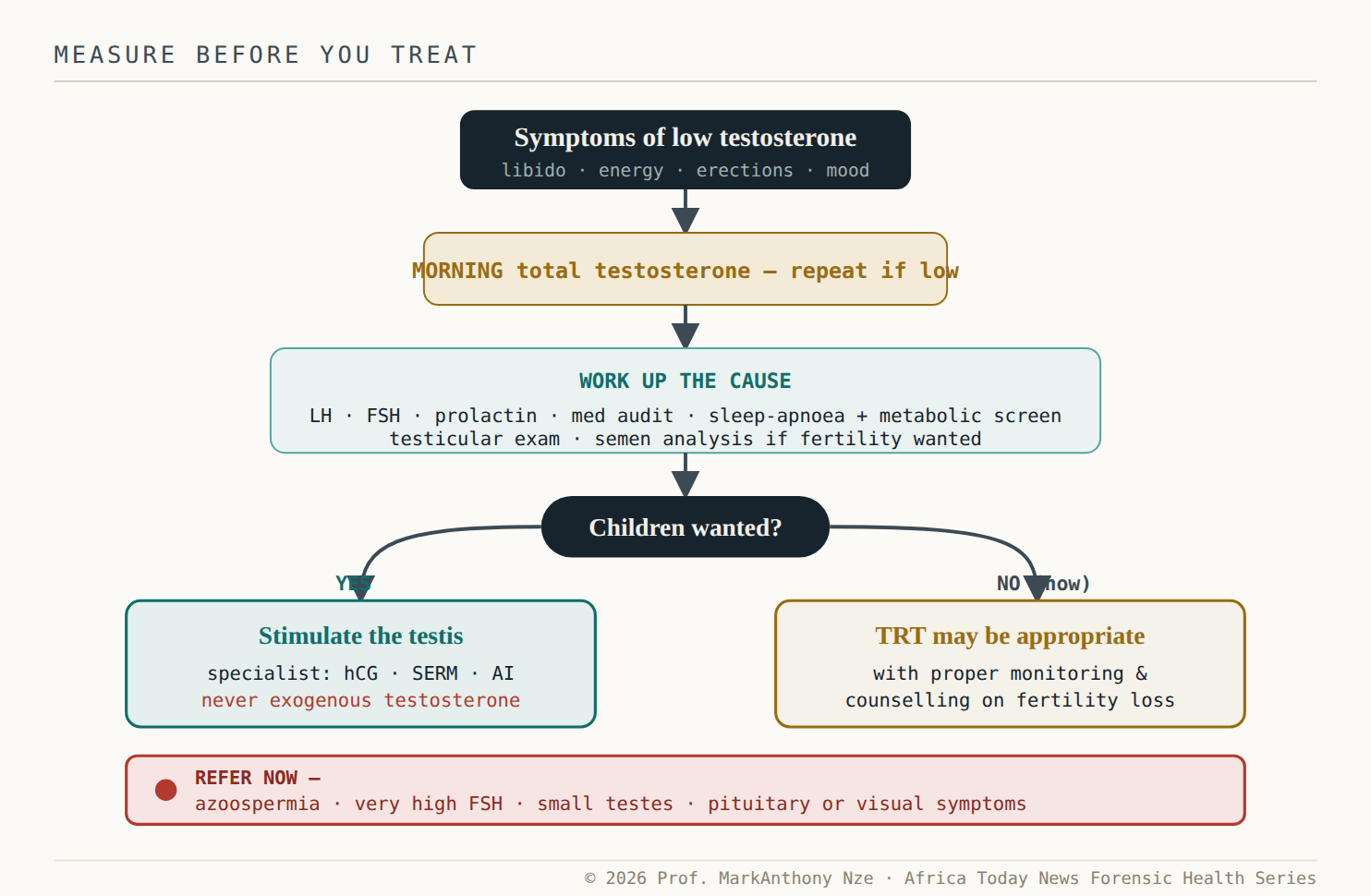
Fig. 21.3 The fork most clinics skip. The single question — does this man want children? — should be asked out loud before a hormone is chosen, because it changes the treatment entirely.
When treatment is warranted and fertility must be protected, the discipline is different from bodybuilding culture in kind, not degree. A reproductive urologist tries to make the testis keep working rather than replace its signal from outside — restoring endogenous production with gonadotropins such as hCG, or with selective estrogen receptor modulators and aromatase inhibitors in selected cases. One approach asks the testis to keep asking; the other trains the pituitary to fall silent. Men hear the word “testosterone” and think strength. The testis only hears feedback.
⚠ Red Flag · Disclosure
Secret hormone use turns a fertility problem into a deception. A woman may endure ovulation tests, painful imaging, medication, and family blame while her partner quietly injects a drug that is suppressing his sperm. Every fertility intake must ask both partners, in plain words, about testosterone, anabolic steroids, SARMs, prohormones, and gym products — and every low-testosterone consultation must ask the man whether he wants children now or later.
Two further cautions close the file. First, men already on prescribed testosterone should not stop abruptly on their own; recovery of sperm production after stopping is real but unpredictable, sometimes taking many months and sometimes needing specialist help, and the honest move is disclosure and a plan, not a panicked halt. Second, erectile dysfunction must never be collapsed into “low testosterone,” because it is one of medicine’s most useful early warnings. The Princeton IV consensus is now explicit that ED should be treated as a marker of cardiovascular risk until proven otherwise — a signal of the same endothelial disease that later announces itself in the heart. A man handed testosterone for what is in fact vascular ED has been sold the easier story and denied the more important one.
The natural plan, then, promises no transformation. It aims for repaired sleep, treated apnoea, less abdominal fat, controlled glucose, disciplined alcohol, and a clean medication list — slower than an injection, and without deliberately silencing the signals that fertility depends on. If testosterone is still genuinely low after all of that, the man has a cleaner case for specialist care and cleaner evidence protecting both his sexuality and his fertility. Measure first. Name the cause. Protect the sperm. Refuse any shortcut that flatters the number in the tube while the testis goes quiet.
The demand · what this file requires
- To fertility clinics —stop testing the woman while the man’s semen goes unexamined. A blocked tube and a low sperm count are found the same way: by looking. Order a baseline semen analysis and a plain medication history from both partners at intake.
- To the supplement and “booster” trade —a product sold for masculinity that raises the blood number while it can suppress sperm is a fertility risk, not a wellness aid. Disclose reproductive effects on the label, or withdraw the claim. Undeclared drug-like compounds in these products are a documented regulatory problem, not a rumor.
- To “men’s clinics” and prescribers —the guideline is not ambiguous: for a man who wants children now or later, exogenous testosterone is the wrong tool. Ask every patient whether he wants children before a hormone is chosen, and record the answer.
- To the man himself —measure first, name the cause, protect the sperm. Refuse any shortcut that flatters the number in the tube while the testis goes quiet — and disclose to your partner what you are taking.
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloguing all underlying source literature, clinical trials, and institutional frameworks (including the World Health Organization, AUA/ASRM, ESHRE, the American Diabetes Association, the U.S. Preventive Services Task Force, FIGO, the U.S. Centers for Disease Control and Prevention, the Pituitary Society, and the Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.