Case File: Female Endocrine
Female Hormones Without Guesswork
“Hormonal imbalance” is not a diagnosis. It is the phrase used when nobody has ordered the tests that would name the real one.
A woman’s menstrual cycle is the most detailed monthly report her body issues, and it is routinely read as if it were a mood. When it comes late, stops, floods, or arrives on no schedule at all, the answer she is most often handed is two words — “hormonal imbalance” — followed by a tea, a supplement, a cleanse, or the advice to relax and wait. None of those words is a diagnosis. Each of them is a way of not ordering the four or five tests that would say what is actually wrong. This chapter is about refusing the vague phrase and demanding the specific one.
Start with what a normal bleed proves. A regular cycle is the visible end of an invisible chain: the hypothalamus releasing GnRH, the pituitary answering with FSH and LH, the ovary ripening a follicle that pours out estrogen, a mid-cycle LH surge that releases the egg, and a corpus luteum that produces progesterone to hold the lining until, if there is no pregnancy, it is shed. A period that comes on time is not merely bleeding; it is a signed statement that the brain, the pituitary, the ovary, and the uterus are all in working conversation. When that statement stops arriving, something in the chain has changed — and the useful question is where, not whether a herb might coax it back.
Read also: The Fertility Repair Series III—Overview
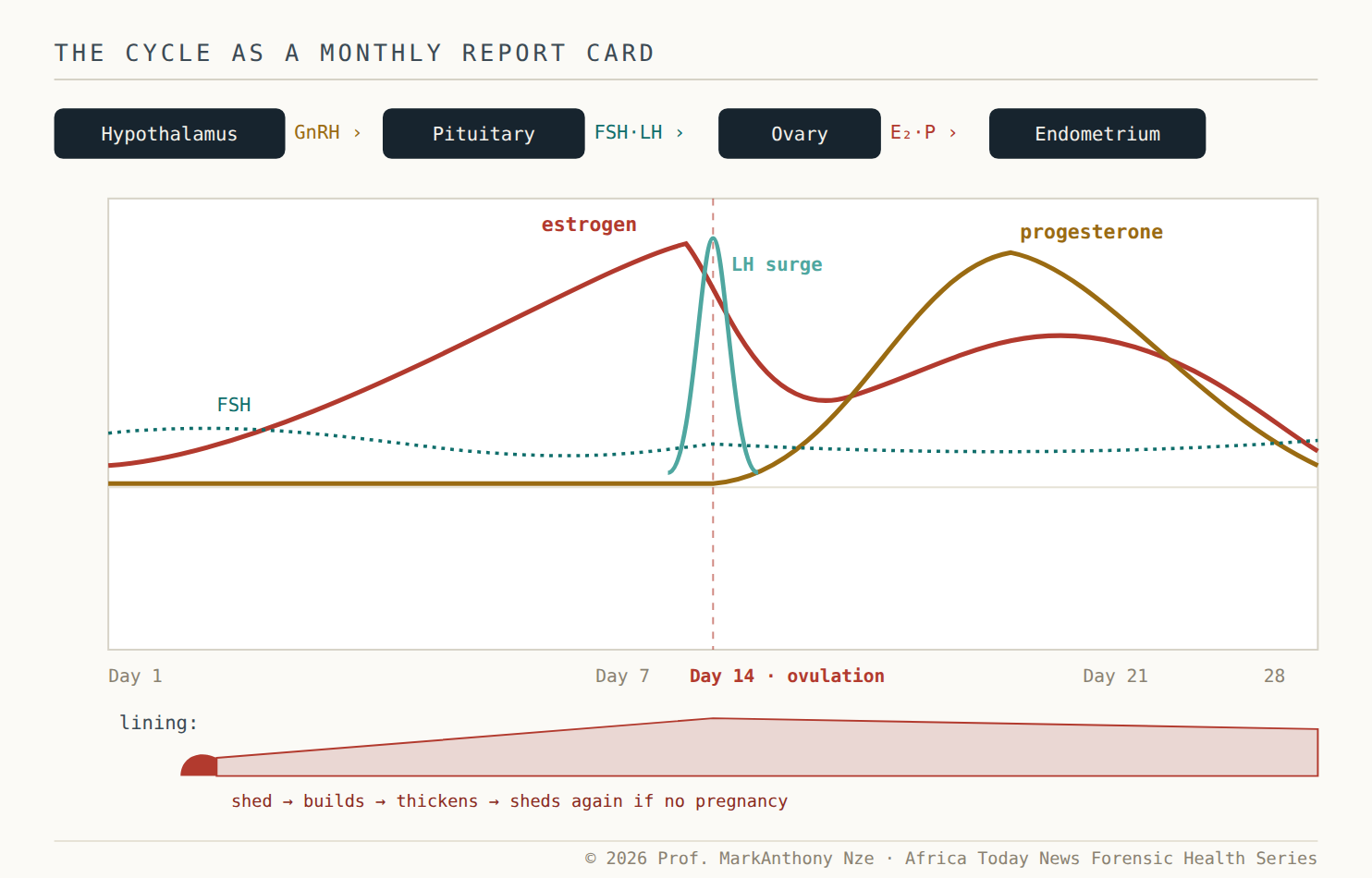
Fig. 22.1 What a regular period proves. A bleed on schedule is the signed end of a four-organ chain. When the schedule breaks, the question is which link — a question tests answer and teas do not.
“Hormonal imbalance” names nothing
The reason the vague phrase survives is that it feels like an explanation while committing to nothing. It cannot be tested, disproven, or acted on. Behind a disordered cycle sits a short, knowable list of real conditions, and each one has a specific test that costs little and settles a great deal. Thyroid disease is checked with a TSH. High prolactin — enough to switch ovulation off entirely — is checked with a single blood draw and, when high, a look at the pituitary. Polycystic ovary syndrome is defined by explicit criteria, not by a feeling. Ovarian insufficiency is read from FSH, estradiol, and anti-Müllerian hormone. And the first cause never to be skipped, because it is common and time-critical, is pregnancy itself, including its dangerous forms. The move that separates medicine from marketing is simply naming which of these it is.
Read also: The Fertility Repair Series III — Part 21
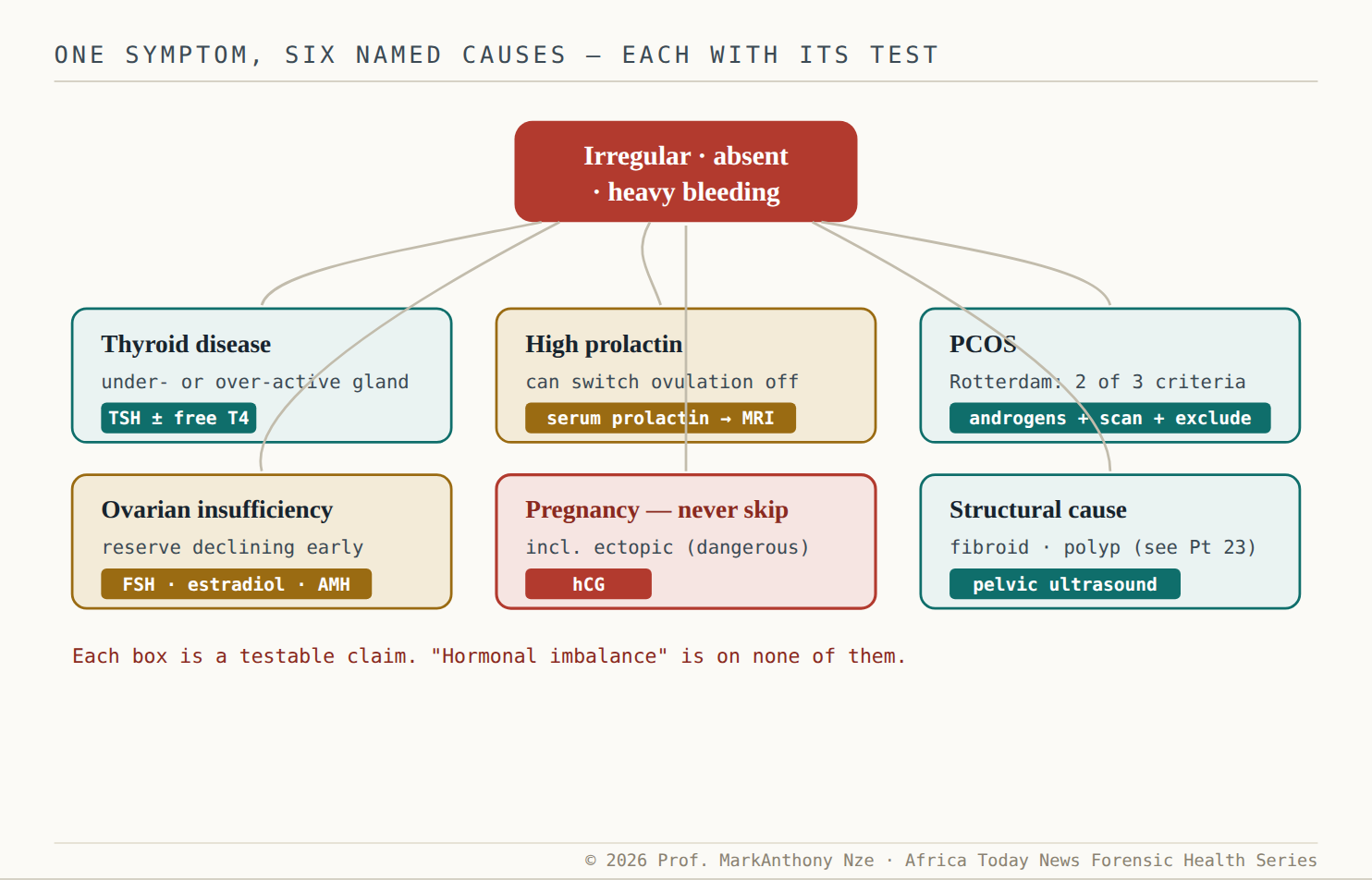
Fig. 22.2 The differential the phrase hides. Six real diagnoses sit behind a disordered cycle, and each carries a cheap, specific test. Naming which one is the entire job.
Take the conditions in turn. Thyroid disease is the quiet saboteur: an under- or over-active gland disturbs ovulation, thickens or thins bleeding, and raises the risk of miscarriage, yet the screening test is inexpensive and widely available. Here the file keeps its discipline, because the evidence does. For overt disease the case for treatment is clear; for the milder, subclinical range the guidance is genuinely unsettled, with reproductive medicine still debating which TSH threshold should trigger treatment and how much treating it changes outcomes. That uncertainty is not a reason to reach for a supplement; it is a reason to test, interpret the number properly, and treat on evidence rather than on a slogan.
High prolactin is the cause most often missed and most easily proven. The hormone that fills the breast after birth, when elevated at the wrong time, suppresses the signals that drive ovulation — so periods space out or vanish, and sometimes the breast leaks milk without a baby. A single blood test finds it; when it is high, imaging looks for a small, usually benign pituitary tumour. The treatment is medical, not surgical in most cases: dopamine-agonist tablets, with cabergoline the preferred agent, lower the hormone, shrink the tumour, and restore ovulation and fertility in the great majority of patients. A woman told to relax and wait, when a prolactin level would have ended the mystery in a day, has been failed by the guess.
PCOS: criteria, not a vibe
Polycystic ovary syndrome is the most common hormonal disorder of reproductive-aged women and the most abused label in the marketplace, applied to anyone with acne, weight, or an off-schedule cycle. Real diagnosis follows the Rotterdam rule — at least two of three features: irregular or absent ovulation, clinical or blood evidence of excess androgens, and the ovarian appearance on ultrasound (or a high AMH) — and, crucially, only after the mimics are excluded by checking thyroid, prolactin, and 17-hydroxyprogesterone. That last step matters because rapid masculinisation or a very high androgen level points away from PCOS toward a tumour or an adrenal disorder, which is a different and more urgent file.
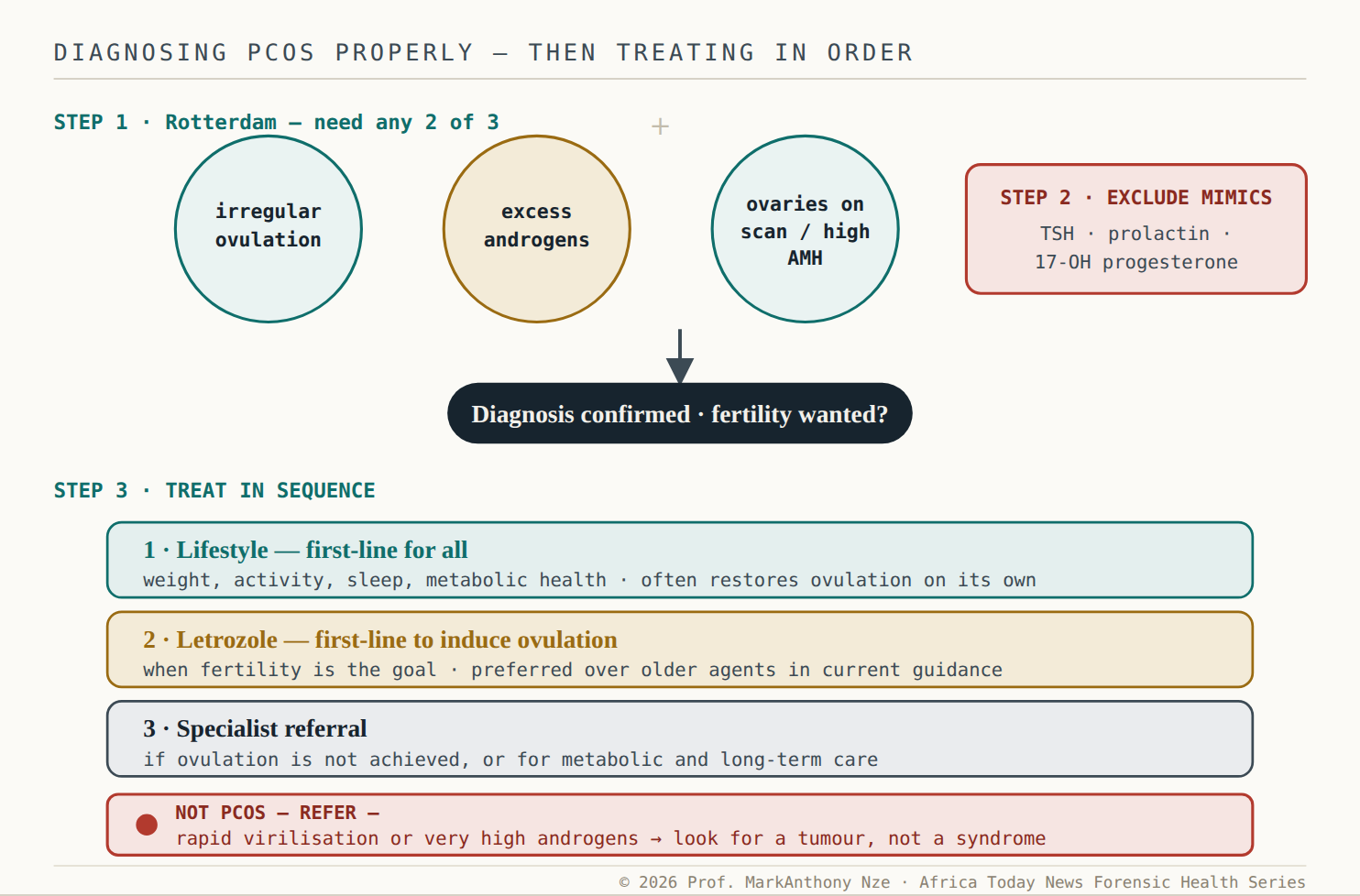
Fig. 22.3 Criteria, then a sequence. Two of three features, mimics excluded — then treat in order: lifestyle, letrozole for ovulation, referral. The red bar marks the case that only looks like PCOS.
The treatment sequence rewards patience over shortcuts. For PCOS, lifestyle change is genuinely first-line and is not a consolation prize — modest weight loss and better metabolic health restore ovulation for many women without a single tablet. When fertility is the goal and ovulation still does not come, current guidance places letrozole first among ovulation-inducing medicines, ahead of the older drug most people have heard of. None of this is a cleanse, a detox, or a “womb-warming” tea. It is a named condition, a defined set of criteria, and an ordered plan — the exact opposite of the guess.
⚠ Red Flag · Do Not Wait
Some bleeding is an emergency, not a cycle problem. A positive pregnancy test with one-sided pain, shoulder-tip pain, dizziness or fainting can mean an ectopic pregnancy, which is life-threatening and needs care the same day. Soaking through a pad an hour, bleeding between periods after 40, or bleeding after menopause are all reasons to be seen promptly, not to start a supplement. When in doubt, the safe move is a clinic, not a shop.
The through-line is simple enough to hold onto in any consulting room. A period is information. When it changes, that information deserves a test with a name attached — TSH, prolactin, androgens, FSH and AMH, an hCG, an ultrasound — not a phrase that explains nothing and sells something. “Hormonal imbalance” is where the investigation stops. The named diagnosis is where care begins.
The demand · what this file requires
- To clinicians —a disordered cycle is a workup, not a phrase. Retire “hormonal imbalance” as a diagnosis and order the specific tests: hCG, TSH, prolactin, androgens, and FSH/AMH where indicated.
- To the supplement, “detox,” and womb-cleanse trade —no tea shrinks a pituitary tumour, corrects a thyroid, or induces ovulation in PCOS. Stop selling cycle “balance” as a substitute for a prolactin level or an ultrasound.
- To anyone using the PCOS label —PCOS is a Rotterdam diagnosis with mimics excluded, not a catch-all for acne and weight. Apply the criteria, exclude thyroid, prolactin, and adrenal causes, and rule out a tumour when androgens are very high.
- To the woman herself —your period is data, and you are owed its reading. Ask for the test by name, and treat bleeding with warning signs as a same-day clinic visit — not a shopping list.
Methodological Note: Documentary evidence presented throughout this forensic series is derived from publicly accessible judicial records, statutory instruments, official government publications, international human rights documentation, sanctions authorities, and verified public reporting. This note applies uniformly to every Part of this volume; it is stated once here rather than repeated after each Part.
A complete Evidentiary Source Index—cataloguing the principal legal authorities, court records, statutory instruments, government documents, sanctions materials, and institutional sources relied upon throughout this volume—is provided at the conclusion of the publication, followed by an Evidentiary Exhibit Appendix.