
Why Women Struggle To Conceive
Infertility is not a mystery when the clock, tube, ovary, uterus, thyroid, and sperm are investigated together.
Monthly bleeding can create false reassurance. A woman may menstruate and still ovulate irregularly, ovulate late, carry tubal damage, live with endometriosis, face sperm-related failure from her partner, or lose embryos for reasons never visible on a calendar. Fertility is not proven by a period. Bleeding is one clue in a longer chain.
Age imposes a biological timetable that polite speech often softens into uselessness. ASRM guidance generally supports evaluation after 12 months of regular unprotected intercourse for women under 35 (Practice Committee of the American Society for Reproductive Medicine, 2021), after 6 months for women 35 or older, and earlier when risk factors exist. That timing is designed to prevent avoidable loss, not to frighten women.
Ovulation sits near the front of the investigation. Irregular cycles may point toward PCOS, thyroid disease, high prolactin, hypothalamic dysfunction, premature ovarian insufficiency, low energy availability, excessive exercise, obesity-linked endocrine disruption, medication effects, or chronic stress physiology. PCOS deserves special attention because insulin resistance, androgen excess, irregular ovulation, sleep-apnea risk, and metabolic disease can occupy the same patient at once.
Read also: The Fertility Repair Series—Part 2
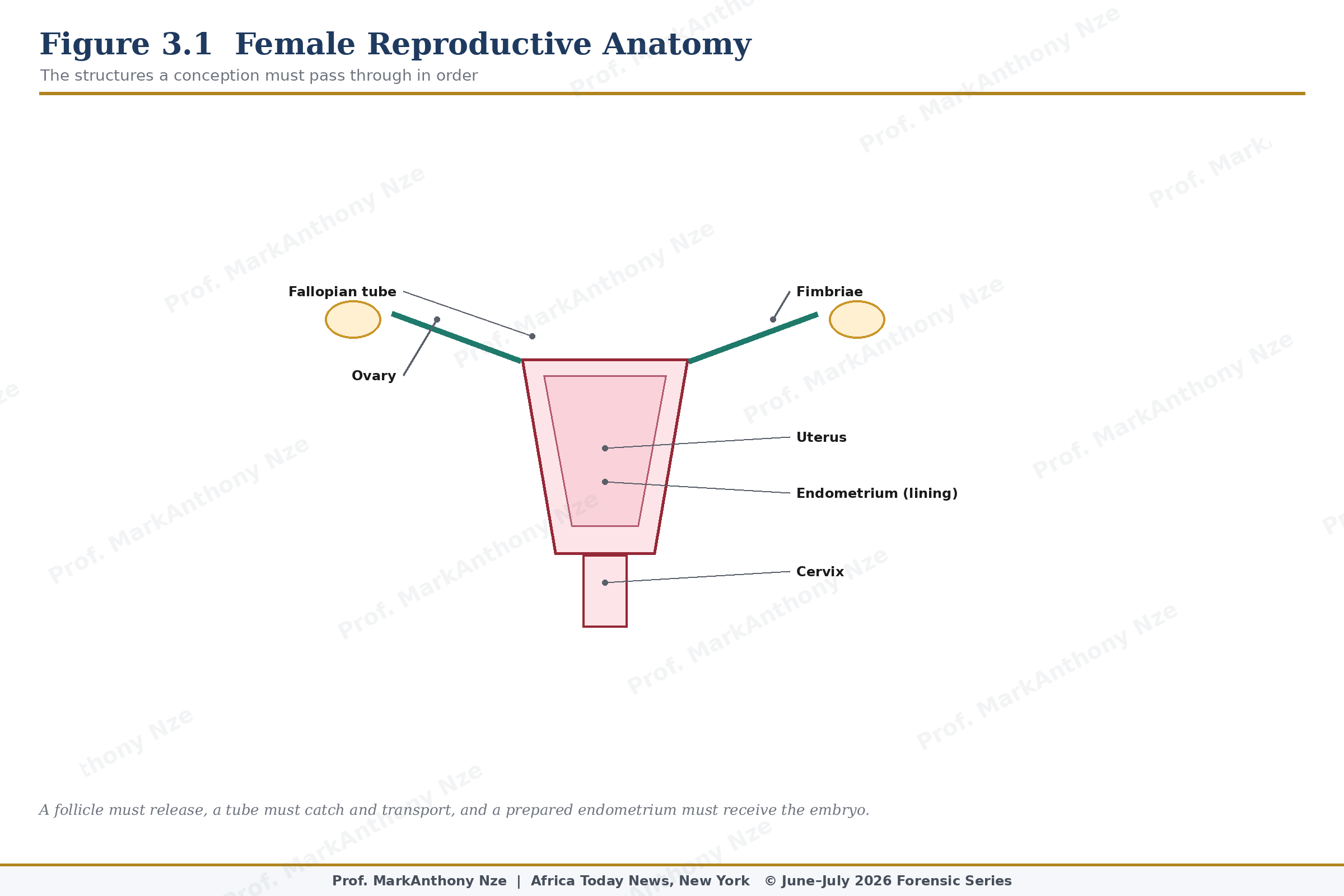
Figure 3.1. Female Reproductive Anatomy.
Fallopian tubes are less forgiving than hormones. Sperm and egg must meet, and the early embryo must travel. A tube scarred by pelvic inflammatory disease, untreated chlamydia or gonorrhea, ectopic pregnancy, surgery, adhesions, ruptured appendix, or endometriosis may block conception or increase ectopic risk. Natural remedies cannot confirm tubal patency. Imaging and specialist evaluation do that work.
Read also: The Fertility Repair Series—Part 1
Endometriosis must be treated as disease, not dramatic menstruation. Symptoms can include severe menstrual pain, deep pain with sex, chronic pelvic pain, bowel or urinary pain around menstruation, fatigue, and infertility; some women have limited symptoms despite meaningful disease. ESHRE guidance addresses diagnosis, pain treatment, infertility care, recurrence, and management because endometriosis can affect pelvic anatomy and inflammatory signaling.
Uterine factors require anatomy, not guessing. Submucosal fibroids, cavity-distorting fibroids, endometrial polyps, intrauterine adhesions, congenital anomalies, and chronic endometrial problems may interfere with implantation or pregnancy continuation. Fibroid size alone is not enough; location and cavity distortion matter. A woman with heavy bleeding, anemia, repeated loss, or known fibroids deserves imaging interpreted through fertility relevance.
Ovarian reserve is another point of confusion. Low reserve does not always mean immediate infertility, and normal reserve does not guarantee a baby, but the information changes counseling. Age, AMH, antral follicle count, prior ovarian surgery, chemotherapy exposure, endometrioma surgery, and family history may alter urgency. Natural remedies should not be used to hide a declining timeline.
Endocrine disease can appear as menstrual disorder, infertility, miscarriage risk, fatigue, galactorrhea, weight change, temperature intolerance, acne, hirsutism, headaches, visual symptoms, or no obvious symptom at all. Thyroid dysfunction can disrupt ovulatory physiology, and prolactin excess can suppress reproductive hormone signaling. Herbal hormone balancing should not precede basic evaluation when symptoms are visible.
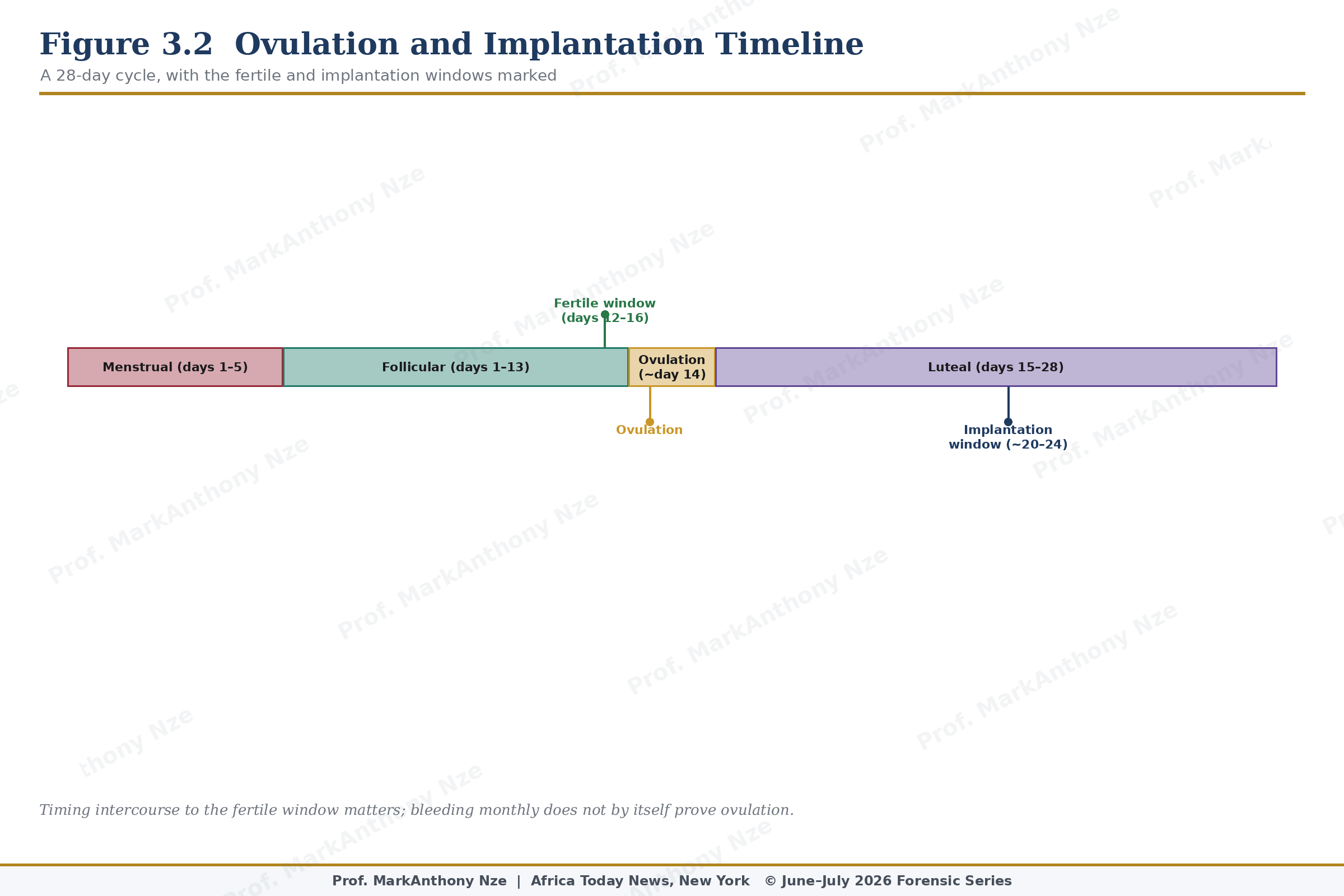
Figure 3.2. Ovulation And Implantation Timeline.
Thyroid and prolactin deserve plain language. A thyroid gland that runs too low or too high can disturb cycles and ovulation, while excess prolactin can reduce gonadotropin signaling and interfere with reproductive rhythm. Nipple discharge outside pregnancy, irregular cycles, headaches, visual changes, unexplained fatigue, or marked temperature intolerance should not be treated as mood. Laboratory evidence belongs in the room.
Male-factor infertility must be pulled into every female-infertility article because women are still blamed too often for a couple’s failure to conceive. Ejaculation does not prove sperm concentration, motility, morphology, vitality, or DNA integrity. A partner with obesity, smoking exposure, heat exposure, diabetes, varicocele, testosterone use, anabolic steroids, prior infection, chemotherapy, or ED belongs in the same diagnostic file.
Miscarriage history must be treated with respect. One early loss is common and may not signal recurrent disease, but repeated loss changes the file. Uterine anatomy, age-related chromosomal risk, thyroid dysfunction, diabetes, antiphospholipid syndrome, genetic factors, and other conditions may require evaluation. Telling a woman to try again without context may be comforting to the speaker and useless to the patient.
Natural care can support female fertility when aimed correctly. Nutrient sufficiency, folic acid supplementation, moderate exercise, smoking cessation, alcohol reduction, healthy body composition, glucose control, sleep repair, and cycle literacy are sensible preconception measures. None should be described as guaranteed conception tools. Better health can improve conditions for reproduction; it does not cancel anatomy, age, severe endometriosis, tubal occlusion, ovarian reserve decline, or male-factor disease.
Fertility timing is often mishandled. Intercourse should occur in the fertile window, but obsession can injure the couple’s sexual relationship. Cervical mucus observation, LH testing, cycle tracking, and intercourse every one to two days during the fertile window can help many couples. App predictions alone can mislead women with irregular cycles because algorithms do not ovulate; bodies do.
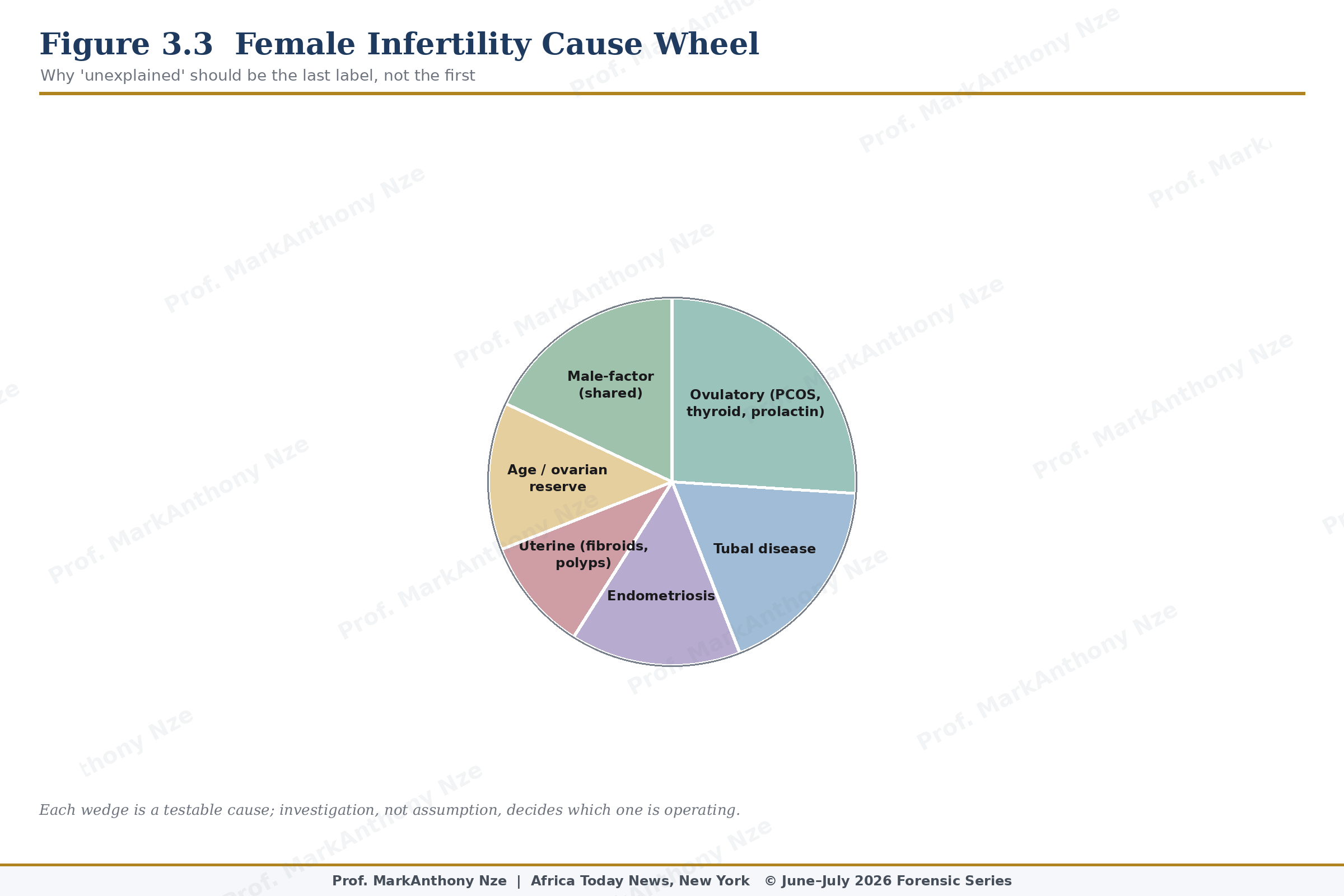
Figure 3.3. Female Infertility Cause Wheel.
Painful sex changes the file. Deep dyspareunia may suggest endometriosis, pelvic adhesions, pelvic-floor guarding, infection, ovarian pathology, or other pelvic disease. Superficial pain may suggest vulvodynia, vaginismus, hormonal tissue change, infection, dermatologic disease, trauma response, or pelvic-floor dysfunction. Pain can reduce intercourse frequency, impair timing, and signal disease that deserves examination. A fertility plan that ignores sexual pain is incomplete.
Food and weight advice must avoid humiliation. Underweight women, women with disordered eating, women with PCOS, women with obesity, athletes with low energy availability, and women recovering from pregnancy loss need different recommendations. A fertility plate is not a punishment; it is a metabolic tool. Protein adequacy, fiber, micronutrients, stable glucose, and enough energy intake matter because the reproductive axis reads scarcity and excess as stress.
Cultural pressure converts infertility into secrecy. Women are pushed toward private blame, public silence, and unregulated remedy markets. Families may demand pregnancy while refusing medical reality. Partners may avoid semen testing. Religious or social shame may delay evaluation until age has narrowed options. Medical journalism has to confront those pressures because misinformation thrives where people cannot speak openly.
Accurate advice is not cruel. Cruelty lies in telling a 39-year-old woman with irregular cycles to wait another year, telling a woman with disabling menstrual pain that suffering is normal, telling a couple to buy more supplements before semen analysis, or telling a patient with suspected tubal disease that faith alone will open anatomy. Hope is not harmed by evidence.
Female infertility is not solved by slogans. It is approached by identifying which part of the chain has failed, which part can be repaired naturally, which part requires treatment, and which delay can no longer be defended.
A better question replaces the old cruelty. Instead of asking why she is not pregnant, ask what has been measured: ovulation, semen, tubes, uterus, hormones, pain, age, glucose, thyroid, prolactin, and timing. That question does not blame her. It rescues the investigation from superstition.
Clinical urgency is not an insult to womanhood. It is the discipline of respecting ovaries, tubes, uterus, hormones, sperm, and time as physical facts rather than emotional symbols.
Medical access remains uneven, especially for women who need imaging, endocrine testing, or reproductive endocrinology referral. Cost cannot be ignored, but poverty does not make false remedies true. Low-cost steps still matter: semen testing where available, cycle records, blood pressure, basic labs, STI history, pain documentation, and timely referral through any reachable clinic system.
A basic clinic visit should also ask about sexual frequency and feasibility. Some couples do not have intercourse near ovulation because of distance, pain, ED, fatigue, religious timing pressure, or conflict. Fertility failure may then be blamed on organs before the schedule is examined. Sex timing is not romance alone; it is part of the biological route.
Source & Clinical Standards
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloging all underlying source literature, clinical trials, and institutional frameworks (including the WHO, AUA/ASRM, ESHRE, and Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.