Sleep, Testosterone And Ovulation
The reproductive axis does not operate cleanly inside chronic sleep debt.
Sleep is usually treated as lifestyle softness until hormones begin to fail. Reproduction depends on timing, and sleep is one of the body’s strongest timing signals. Testosterone rhythm, cortisol tone, insulin sensitivity, appetite regulation, mood, libido, ovulatory signaling, and vascular repair all respond to sleep quantity and quality. A couple trying to conceive inside chronic sleep debt is asking the reproductive axis to work through metabolic noise.
Male sexual function is especially vulnerable to poor sleep. Short sleep, fragmented sleep, untreated sleep apnea, rotating shifts, late alcohol, and stress-driven insomnia can reduce morning energy, worsen insulin resistance, raise blood pressure, impair mood, and weaken libido. ED may then be blamed on age or anxiety while the patient is repeatedly suffocating at night through obstructive sleep apnea.
Female reproductive rhythm also depends on central timing. Sleep disturbance and circadian disruption can affect gonadotropin signaling, ovulatory regularity, metabolic health, and fertility-treatment outcomes. A woman with irregular cycles, PCOS, obesity, night-shift work, insomnia, or severe stress should not have sleep treated as a footnote. Ovaries receive signals from a brain and body that need rhythmic order.
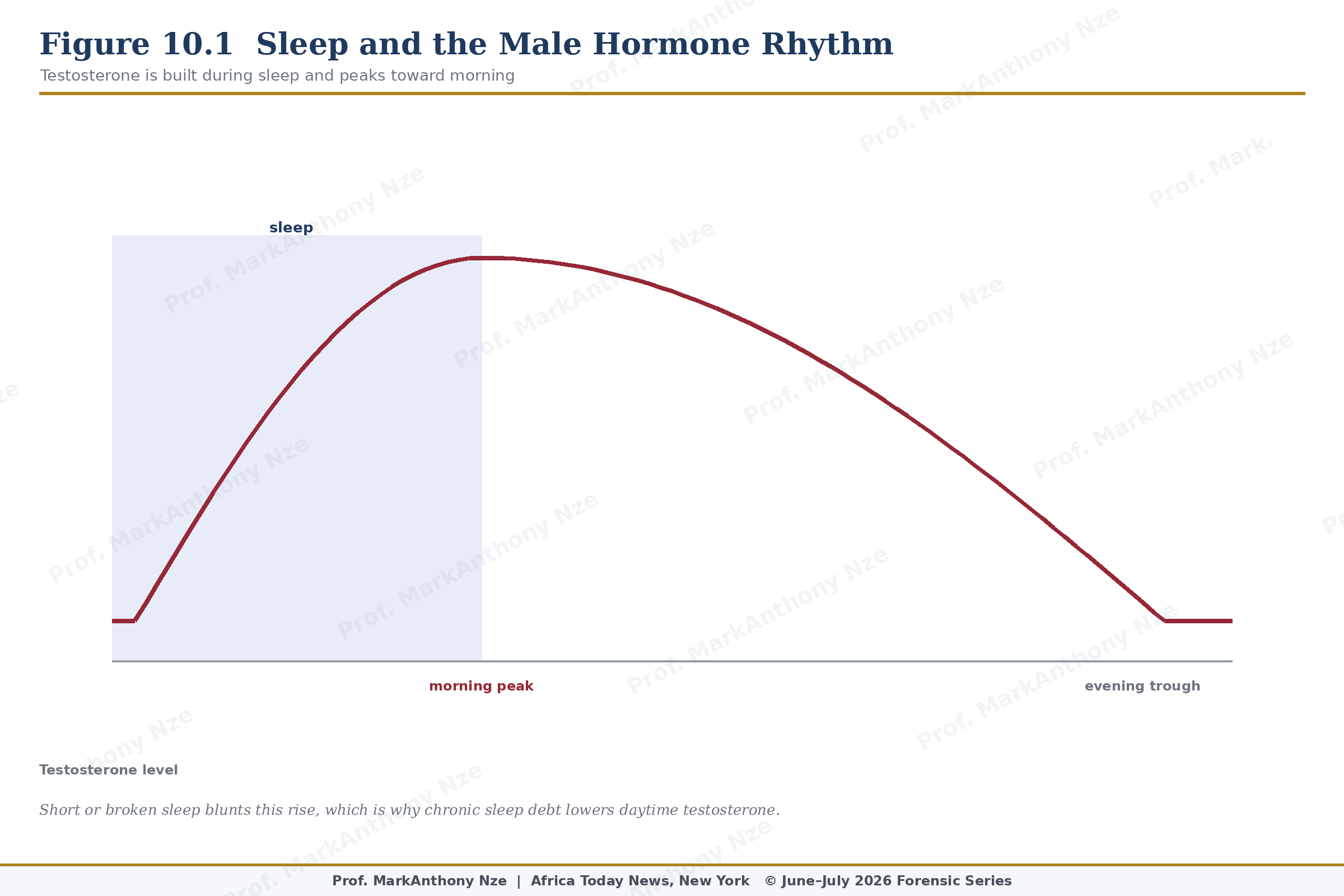
Figure 10.1. Sleep And Male Hormone Rhythm.
Obstructive sleep apnea deserves aggressive suspicion in both sexes. Loud snoring, witnessed pauses, choking awakenings, morning headaches, daytime sleepiness, resistant hypertension, central obesity, and low libido are not minor details. Oxygen dips and sympathetic surges can worsen blood pressure, vascular injury, insulin resistance, fatigue, mood, and sexual function. A sleep study may become a fertility intervention by exposing the nightly injury.
PCOS and sleep can aggravate each other. Women with PCOS have higher risk of sleep-disordered breathing in some populations, and poor sleep can worsen insulin resistance, appetite control, fatigue, and mood. A woman told only to lose weight while nobody asks about snoring receives incomplete care. Sleep repair may not cure PCOS, but ignoring sleep leaves a metabolic driver untouched.
Testosterone should be discussed carefully in this context. Healthy sleep supports normal testosterone rhythm, while sleep loss and untreated apnea can worsen fatigue, libido, mood, and metabolic health. A man may ask for testosterone when the first intervention should be sleep assessment, weight repair, exercise, medication review, and testing only when clinically indicated.
Read also: The Fertility Repair Series—Part 9
Alcohol is a common sleep fraud. It may sedate the brain while fragmenting sleep, worsening snoring, aggravating apnea, reducing REM quality, and impairing next-day energy. Men using alcohol to manage performance fear may deepen ED risk through sleep disruption and hormonal strain. Women drinking to cope with fertility stress may worsen sleep and cycle-related distress. Sedation is not restoration.
Screen exposure and late-night work matter because light and arousal signals delay sleep timing. Phone use in bed, late news, gambling, pornography, work emails, family conflict, and night-time business pressure can keep the nervous system alert when reproductive hormones require order. Advice to sleep earlier sounds simple because the hard part is not information. It is control over the evening.
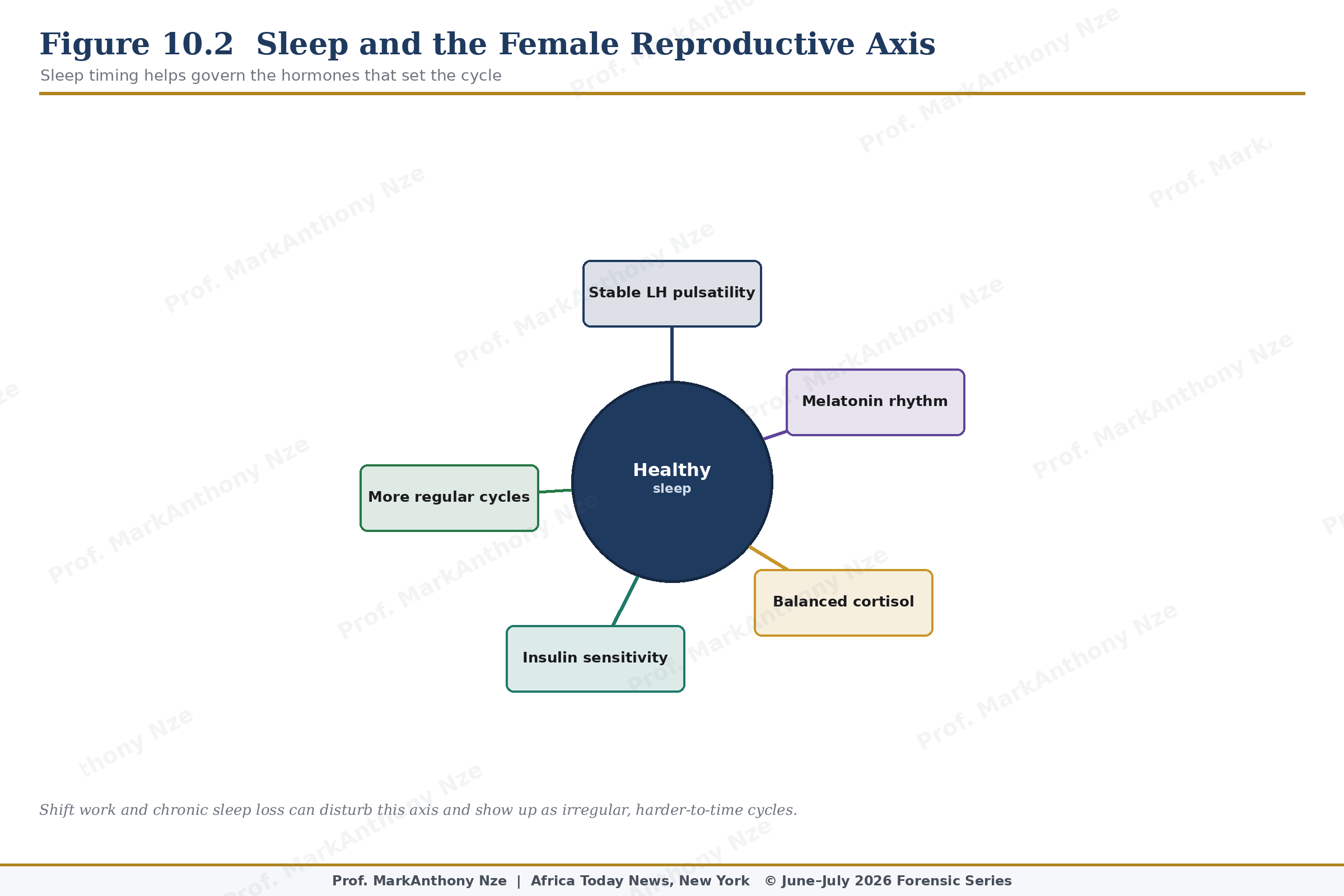
Figure 10.2. Sleep And Female Reproductive Axis.
Shift work creates a harder problem. Nurses, factory workers, security staff, drivers, physicians, hospitality workers, and caregivers may live against the clock. Fertility advice must account for income reality. Regular sleep windows, dark rooms, bright light at planned wake time, reduced caffeine late in the shift, meal planning, and protected recovery days may reduce harm even when the schedule cannot be ideal.