Case File: Uterine Cavity
Fibroids, Polyps and the Uterine Cavity
A fibroid’s size is the first thing everyone asks about and nearly the last thing that matters. Its address inside the uterus decides whether it touches fertility at all.
The first question a woman is asked when a fibroid is found is how big it is, and it is very nearly the wrong question. Fibroids are common, most cause no fertility trouble at all, and a large one growing outward on the surface of the uterus can be entirely irrelevant to conceiving. What decides whether a fibroid matters is not its diameter but its address — specifically, how close it sits to the cavity, the small triangular space where an embryo must implant. A fibroid pressing into that space can quietly wreck implantation; a bigger one facing the other way may do nothing. This chapter is about reading the map, not the measuring tape.
To see why address beats size, picture the uterus in cross-section. Its wall has three layers: a thin outer covering, a thick muscular middle called the myometrium, and an inner lining, the endometrium, that faces the hollow cavity and thickens each month to receive an embryo. A fibroid is a benign knot of that muscle, and where it grows within these layers is exactly what the international FIGO system was built to record. The classification runs from Type 0, a fibroid sitting entirely inside the cavity, through the wall, out to Type 7, dangling off the outer surface — and it exists precisely because “fibroid” alone tells a clinician almost nothing useful about fertility.
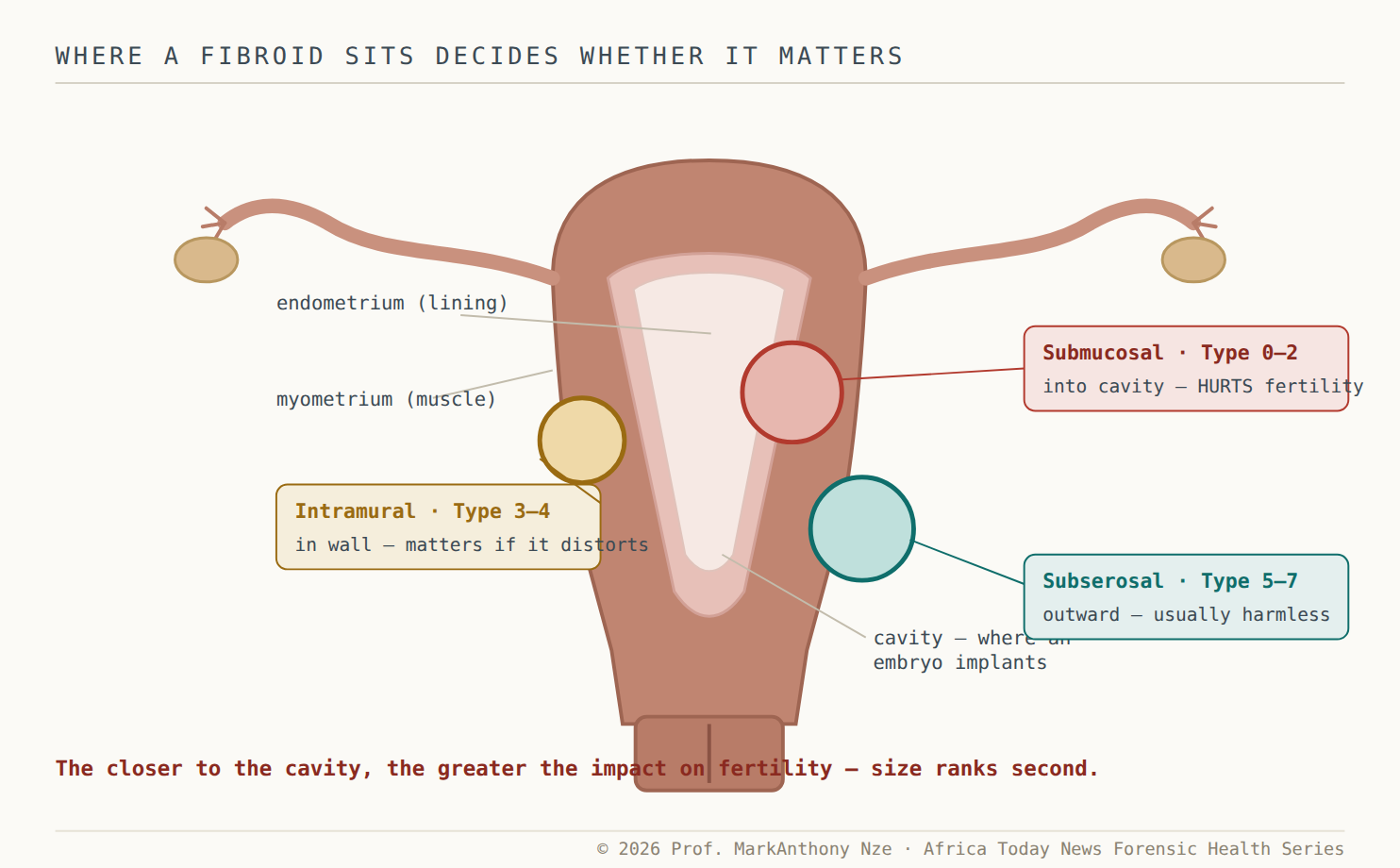
Fig. 23.1 Address, not diameter. The same-size knot of muscle means three different things depending on where it grows. Only the one pressing into the cavity reliably threatens implantation.
Read also: The Fertility Repair Series III — Part 22
The cavity is the ground an embryo lands on
The reason the cavity is sacred is mechanical and biological at once. An embryo must attach to a smooth, receptive lining; anything bulging into that space distorts it, and the evidence that this matters is unusually consistent. Pooled data across many trials show that submucosal fibroids — those pressing into the cavity — sharply lower implantation and clinical pregnancy rates and raise the risk of early miscarriage. Crucially, removing them changes the odds: women who had cavity-distorting fibroids taken out were markedly more likely to conceive than those who left them in place. This is why the ASRM guidance draws its line not around size but around the cavity, finding fair evidence that removing cavity-distorting fibroids improves pregnancy rates and reduces early loss.
The harm is not only the visible bulge. A submucosal fibroid distorts the lining it presses against, disturbs the local blood supply an embryo needs, and provokes low-grade inflammation across the cavity — so the injury extends a little beyond the fibroid’s own footprint. This is also why the size myth is so stubborn and so misleading: a two-centimetre Type 0 fibroid sitting inside the cavity can matter more than an eight-centimetre subserosal one ballooning harmlessly outward. Counselling a woman on the diameter of a fibroid without stating where it sits is close to counselling her on nothing. The measuring tape flatters the wrong number, exactly as an inflated testosterone reading did for men in an earlier chapter.
The same logic indicts a smaller, quieter culprit: the endometrial polyp. A polyp is an overgrowth of the lining itself — often no larger than a grape — that projects into the cavity on a stalk and occupies the very ground where an embryo would otherwise settle. It rarely causes pain and may show only as spotting or as an incidental finding on a scan, which is exactly why it is so often dismissed. But a polyp sitting in the implantation zone is a physical obstacle in a small space, and removing it is a brief, low-risk procedure that can restore a lining to full working order.
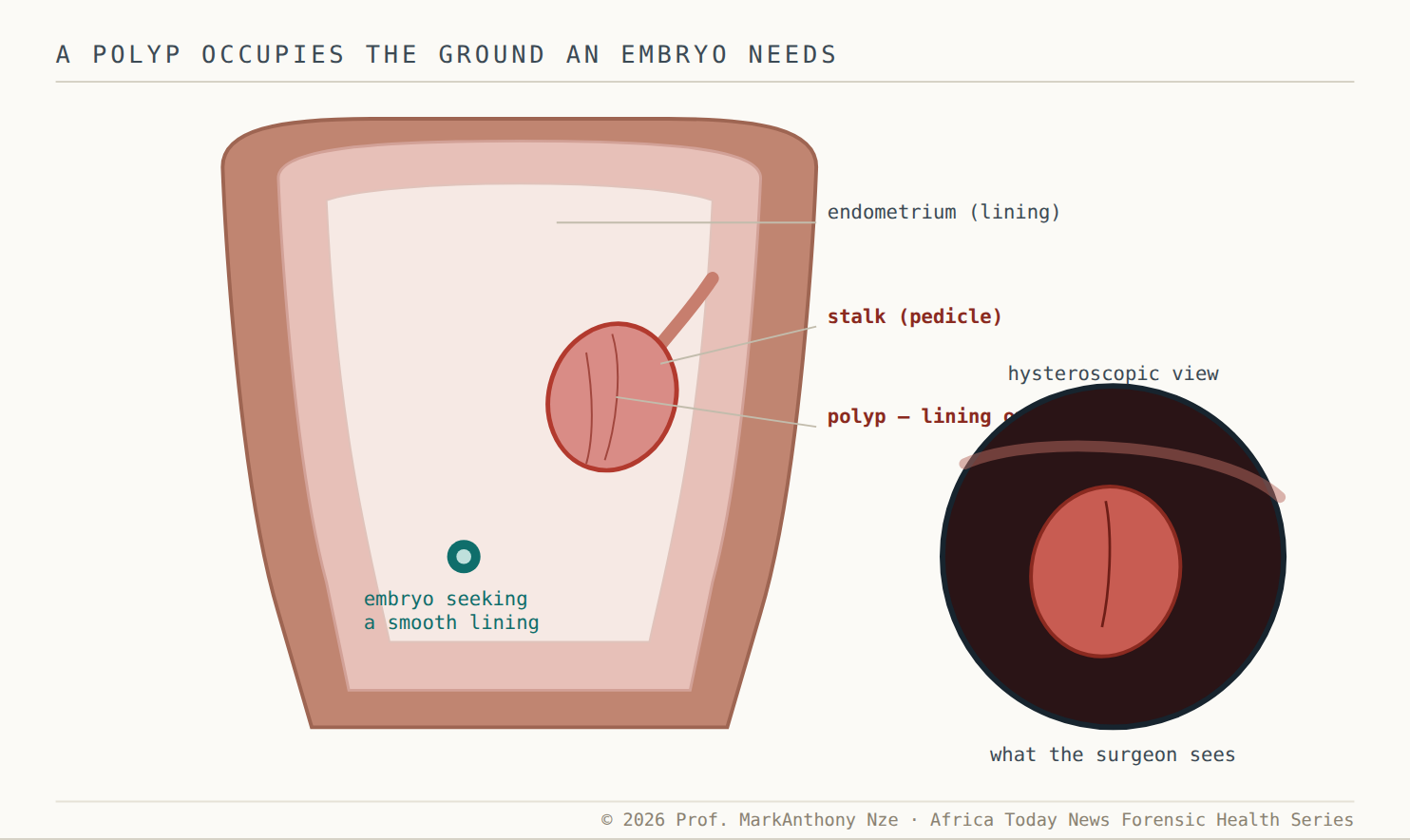
Fig. 23.2 A small obstacle in a small space. A polyp is lining overgrowth on a stalk, sitting where an embryo would implant. Painless, easily missed, and removable in a short hysteroscopic procedure.
Read also: The Fertility Repair Series III — Part 21
See inside before you cut — or before you don’t
None of this can be settled by feel, by a tea, or by a scan read too quickly. Tea cannot reveal whether a fibroid distorts the lining; a supplement cannot tell a Type 2 from a Type 5. The cavity has to be looked at, and there is an orderly way to look. Transvaginal ultrasound comes first and finds most fibroids, but it can miss how far one intrudes into the cavity. Saline poured gently into the uterus during a scan — a saline infusion sonogram — outlines the cavity and exposes a submucosal fibroid or a polyp that a plain scan glossed over. Hysteroscopy, a thin camera passed into the uterus, is the reference standard because it both sees the lesion and, in the same sitting, removes it.
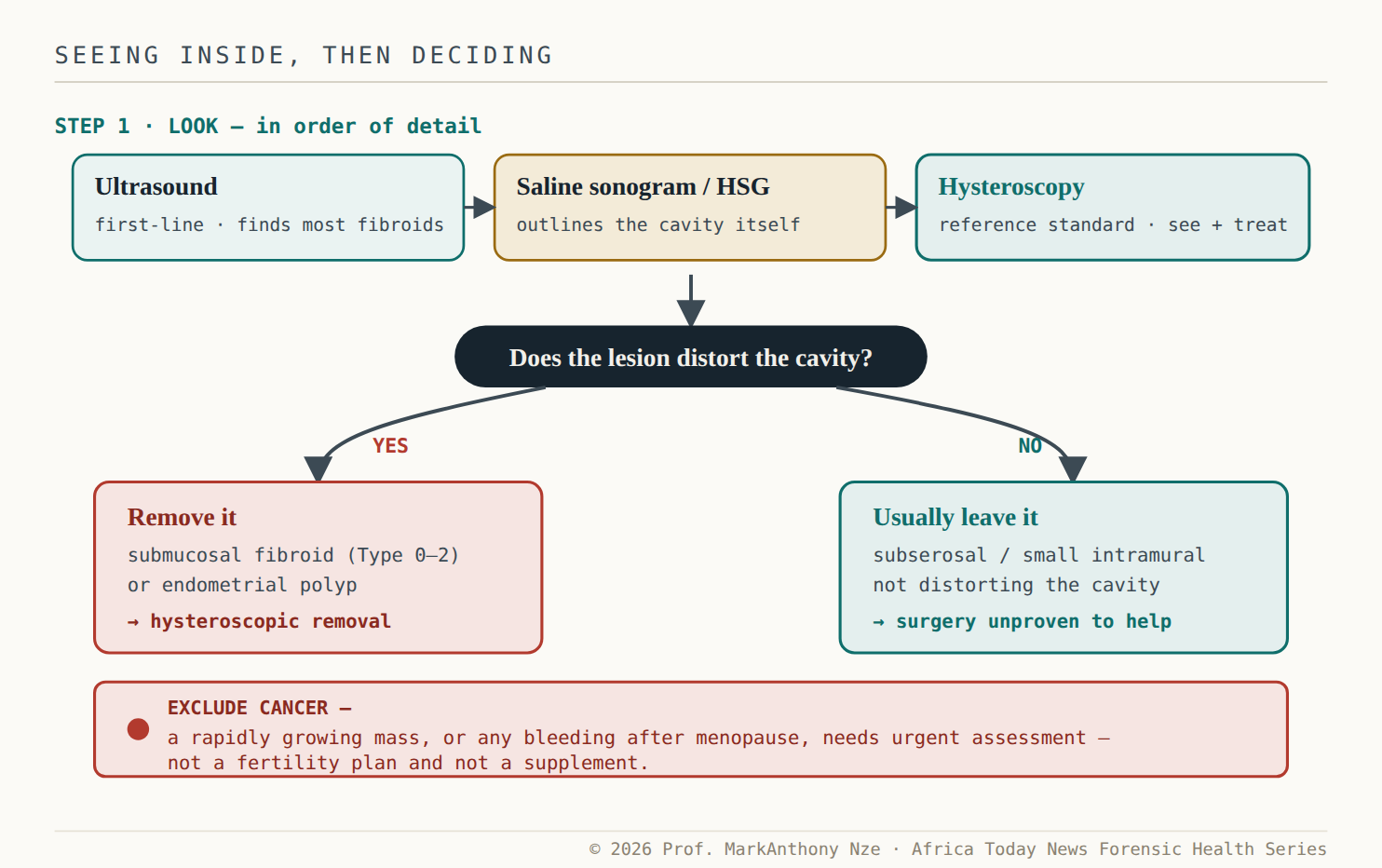
Fig. 23.3 Look first, then decide by the cavity. Distorting lesions come out; lesions that spare the cavity usually stay, because removing them is not proven to help. The red bar is the exception that overrides everything.
That last distinction protects women from unnecessary surgery as firmly as it pushes for the necessary kind. Because the evidence favours removing cavity-distorting lesions but does not support removing fibroids that leave the cavity alone, an operation on a large subserosal fibroid — done in the name of fertility — may carry all the risk of surgery and none of the benefit. The discipline cuts both ways: remove what distorts the cavity, and resist removing what does not. Neither decision can be made without first looking inside.
Red flag · not just fertility
A uterine mass is not always a simple fibroid. A mass that grows quickly, or any bleeding after menopause, can signal something that must be excluded urgently — this is a same-week clinical assessment, not a matter for a womb-cleanse, a fertility tea, or watchful hoping. When the pattern is unusual, the safe move is a specialist, promptly.
Held together, the file reads simply. A fibroid is not a verdict, and its size is not the headline. What matters is whether it — or a quiet polyp beside it — intrudes on the small space an embryo needs. That question is answered by looking, with ultrasound, saline sonography, and hysteroscopy, and it is acted on by removing what distorts the cavity and leaving alone what does not. No herb sees inside the uterus. No cleanse corrects its architecture. The cavity is read, not guessed.
The demand · what this file requires
- To clinicians —stop reporting a fibroid by size alone. Classify it by FIGO type and state plainly whether it distorts the cavity, because that — not the diameter — is what the fertility decision turns on.
- To surgeons —the evidence removes cavity-distorting lesions and spares the rest. Do not operate on a cavity-sparing fibroid in fertility’s name, and do offer hysteroscopic removal for a submucosal fibroid or polyp that distorts the lining.
- To the womb-cleanse and fibroid-tea trade —no herb, seed, or cleanse shrinks a submucosal fibroid, dissolves a polyp, or corrects the cavity. Stop selling “womb detox” as an alternative to looking inside.
- To the woman herself —ask for the cavity to be assessed, by name — ultrasound, then saline sonogram or hysteroscopy. And treat a fast-growing mass or post-menopausal bleeding as a same-week clinic visit, not a shopping list.
Source & Clinical Standards
Note: The data, diagnostics, and clinical benchmarks throughout this series are drawn directly from peer-reviewed medical literature, epidemiological data, and established global healthcare consensus. To protect the narrative rhythm of this digital layout, individual article bibliographies have been unified.
A complete master registry—cataloguing all underlying source literature, clinical trials, and institutional frameworks (including the World Health Organization, AUA/ASRM, ESHRE, the American Diabetes Association, the U.S. Preventive Services Task Force, FIGO, the U.S. Centers for Disease Control and Prevention, the Pituitary Society, and the Princeton IV Consensus)—is compiled in full at the conclusion of the complete volume.